
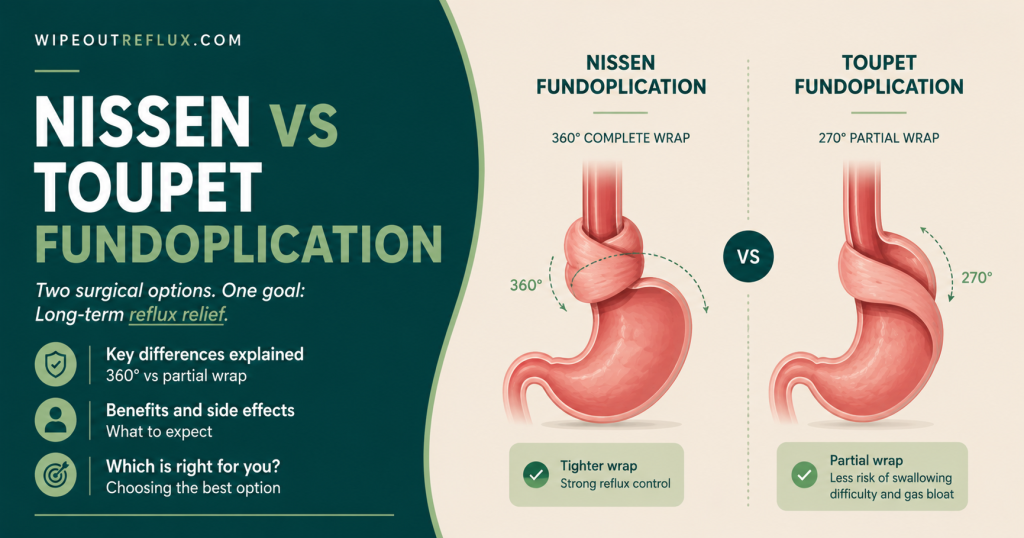
If you are heading toward anti-reflux surgery, you will quickly run into a fork in the road: Nissen or Toupet? Both are laparoscopic fundoplications — operations that reinforce the valve at the top of your stomach to stop reflux — but they differ in one crucial way. Nissen wraps the stomach all the way around the oesophagus (a full 360° wrap), while Toupet wraps it only partway (a 270° partial wrap).
The honest headline is this: the evidence shows they control reflux about equally well, but the Toupet’s partial wrap causes significantly fewer side effects — less difficulty swallowing, less gas-bloat, and less trouble belching. That is why the Toupet has steadily gained favour. The Nissen, though, remains the long-standing gold standard with a slightly tighter valve and the longest track record.
So there is no universal winner — the “better” operation depends on you. I have managed my own LPR for over eight years, so let me break down how the two differ, what the research actually shows, and how surgeons decide between them.
Key Takeaways
- Nissen is a full 360° wrap; Toupet is a partial 270° wrap. Both reinforce the lower oesophageal valve and both include repairing any hiatal hernia.
- Reflux control is comparable. Pooled trial data show no significant difference in heartburn, regurgitation, or acid exposure between the two.
- Toupet has fewer side effects. It causes significantly less dysphagia, gas-bloat, inability to belch, and fewer reoperations.
- Nissen produces a slightly tighter valve (higher sphincter pressure) and has the longer history as the gold standard.
- The old “tailoring” rule has been questioned. Toupet’s lower dysphagia appears to apply broadly, not just to people with weak oesophageal motility.
- The best choice is individualised — based on your anatomy, oesophageal motility, priorities, and your surgeon’s experience.
- Neither operation replaces the fundamentals. Surgery fixes the valve, not your diet or triggers.
The Two Operations Explained
Both procedures share the same foundation. A surgeon works laparoscopically (keyhole surgery), repairs any hiatal hernia by closing the gap in the diaphragm, and then reinforces the valve by wrapping the top of the stomach (the fundus) around the lower oesophagus. The difference is how far around that wrap goes.
Nissen fundoplication (360°)
The Nissen is a complete wrap — the fundus is brought all the way around the oesophagus and stitched to itself, forming a full collar. It is the most widely used and longest-established anti-reflux operation, often called the gold standard. The trade-off is that a full wrap is the tightest, which is what drives its higher rate of side effects.
Toupet fundoplication (270°)
The Toupet is a partial posterior wrap — the fundus is brought around the back of the oesophagus but left open at the front, covering roughly three-quarters of the circumference. It was specifically developed to keep the anti-reflux benefit while reducing the swallowing and bloating problems that can follow a full wrap.
If you want the background on why this valve fails and needs reinforcing in the first place, I cover it in my guide to the stomach sphincter and reflux.
How They Differ Mechanically
Understanding the mechanics explains everything that follows. A full 360° wrap creates a tighter, higher-pressure barrier. That is great for stopping reflux — but it also makes it harder for food to pass through when you swallow, and harder for gas to escape upward when you need to belch. The result can be difficulty swallowing (dysphagia) and trapped gas causing bloating (the “gas-bloat syndrome”).
A partial 270° wrap leaves a little more “give” at the junction. It still reinforces the valve enough to control reflux, but because it is not a complete collar, food passes more easily and gas can vent more readily. That single mechanical difference is why the two operations end up with such different side-effect profiles — and it is the heart of the whole debate.
Reflux Control: Is One More Effective?
This is usually the first question people ask, and the answer is reassuring: for most patients, the two operations control reflux comparably.
A meta-analysis of eight randomised controlled trials found no significant differences between Nissen and Toupet in postoperative heartburn, regurgitation, acid exposure (DeMeester scores), or oesophagitis. The main measurable difference in favour of Nissen was a slightly higher lower-oesophageal-sphincter pressure and a shorter operating time [Du et al., BMC Gastroenterology, 2016].
It is worth being honest about the history here: some older studies raised a concern that a partial wrap might allow slightly more heartburn to recur over the long term. But the larger, pooled randomised evidence has not borne that out — reflux control comes out broadly equal. So while the Nissen creates a marginally tighter valve on paper, that has not translated into meaningfully better real-world reflux control for most people.
Side Effects: Where They Really Diverge
If reflux control is a tie, side effects are where the Toupet pulls ahead — and this is the crux of why practice has shifted.
A meta-analysis of 13 randomised trials found that while the two operations were equally effective, the rates of dysphagia, gas-bloat syndrome, inability to belch, and reoperation for severe dysphagia were all significantly higher after the full Nissen wrap [Tian et al., PLoS One, 2015]. The Du analysis reached the same conclusion, with more dysphagia, gas-bloating, inability to belch, dilatation for dysphagia, and reoperation after Nissen [Du et al., BMC Gastroenterology, 2016].
In plain terms: with a Toupet, you are less likely to struggle swallowing, less likely to feel bloated and unable to burp, and less likely to need a second procedure to loosen things up. For a lot of people, that tips the balance.
The “Tailored Approach” Debate
For years, surgeons followed a rule of thumb: if a patient had weak oesophageal muscle (poor motility), give them a Toupet rather than a Nissen, on the logic that a full wrap would be too much for a sluggish oesophagus to push food through, causing dysphagia. This was called “tailoring” the wrap to the patient’s manometry (a test of oesophageal muscle function).
Then a well-known randomised trial challenged that thinking. It stratified patients by their oesophageal motility and randomised them to Nissen or Toupet. Dysphagia (27% versus 9%) and chest pain on eating (22% versus 5%) were both significantly more common after the Nissen — but crucially, there was no difference in outcomes between the good-motility and poor-motility groups. The authors concluded there was no reason to tailor the degree of wrap to preoperative manometry [Booth et al., British Journal of Surgery, 2008]. In other words, the Toupet’s swallowing advantage seemed to apply to everyone, not just people with weak motility. A separate randomised trial also examined this tailored concept in 200 patients stratified by motility [Strate et al., Surgical Endoscopy, 2008].
Where does that leave things? Practice still varies by surgeon, and many still lean toward a partial wrap when motility is clearly poor. But the evidence has pushed the field toward considering the Toupet more broadly, rather than reserving it only for dysmotility.
At a Glance: Nissen vs Toupet
Here is the head-to-head in simple terms.
- Wrap: Nissen is a full 360° wrap; Toupet is a partial 270° posterior wrap.
- Reflux control: Comparable for both, based on pooled randomised data.
- Valve pressure: Slightly higher with Nissen.
- Dysphagia (difficulty swallowing): Higher with Nissen; lower with Toupet.
- Gas-bloat / trouble belching: More common with Nissen; less with Toupet.
- Reoperation for side effects: Higher with Nissen.
- Track record: Nissen is the longer-established gold standard.
- Overall trend: Toupet increasingly favoured for its side-effect profile with equivalent reflux control.
So Which Is Better?
Here is my honest read of the evidence. If you judge purely by reflux control, it is essentially a tie. Once you factor in side effects, the Toupet has the edge for most people — comparable reflux control with less dysphagia, less gas-bloat, and fewer reoperations. That is exactly why many surgeons and recent analyses now lean toward the partial wrap as a sensible default.
But “better for most” is not “better for everyone.” The Nissen remains a superb, durable operation with the longest track record, and some surgeons prefer its tighter valve for patients with particularly severe reflux or specific anatomy. And the single biggest variable is often not the technique itself but the experience of the surgeon performing it — a well-done Nissen beats a poorly done Toupet every time.
The practical takeaway: this is a decision to make with an experienced anti-reflux surgeon, weighing your reflux severity, your oesophageal motility, your anatomy, and what matters most to you. If avoiding swallowing trouble and bloating is a high priority, the Toupet’s profile is appealing; if maximal barrier strength is the goal, the Nissen still earns its gold-standard reputation.
Where Surgery Fits — and the Alternatives
Before either operation, remember that surgery is generally reserved for proven, refractory reflux — confirmed on testing, not just assumed from symptoms. If your medication is only partly helping, it is worth understanding why first, because some causes are fixable without an operation; I cover them in acid reflux medication not working. And confirming that reflux is genuinely behind your symptoms matters enormously, especially with silent reflux — see GERD vs LPR.
Full fundoplication is also not the only surgical route anymore. Less invasive options like the Stretta procedure and other reflux surgery options sit alongside Nissen and Toupet on the treatment ladder, and the right rung depends on your situation. If your aim is simply to get off medication, read about getting off PPIs and acid rebound before making any big decisions.
Whichever path you consider, the foundation still matters. Surgery reinforces the valve, but it does nothing to change what you eat or how you eat — and those triggers keep shaping how you feel. That is exactly what my Wipeout Diet Plan is built to address.
Conclusion
Nissen versus Toupet is one of the longest-running debates in reflux surgery, and the evidence has brought it into fairly clear focus. On reflux control, the two are comparable — a full wrap and a partial wrap both do the core job well. Where they part ways is side effects, and here the Toupet’s 270° partial wrap consistently causes less dysphagia, less gas-bloat, and fewer reoperations than the full 360° Nissen. That is why the partial wrap has steadily gained ground, and why the old idea of reserving it only for people with weak oesophageal motility has been questioned.
Still, the Nissen remains a durable, proven gold standard, and the “better” operation genuinely depends on your reflux severity, your anatomy, your priorities, and — perhaps most of all — the skill of your surgeon. This is a decision to make together with an experienced specialist after proper reflux testing, not a verdict to reach from an article.
And whatever you decide, do not overlook the groundwork. In my experience, the people who do best are the ones who get their diet and habits right, whether or not they have surgery — because those are the triggers no wrap can fix. That is exactly what my Wipeout Diet Plan is designed to deliver, in the depth this condition needs, and the Wipeout Food Reference Guide is the essential companion that shows exactly which foods and drinks are reflux-friendly and their pH values. Get that foundation right first — for many people, it changes everything.
Frequently Asked Questions
Is Nissen or Toupet better for acid reflux?
They control reflux comparably, according to pooled randomised data. The Toupet (partial 270° wrap) causes fewer side effects — less dysphagia and gas-bloat — so it is often preferred, while the Nissen (full 360° wrap) offers a slightly tighter valve and the longest track record. The best choice is individualised.
What is the main difference between Nissen and Toupet fundoplication?
The extent of the wrap. Nissen wraps the stomach fully around the oesophagus (360°), creating a tighter valve. Toupet wraps it only partway around the back (270°), leaving more give at the front, which reduces swallowing difficulty and bloating.
Does the Toupet control reflux as well as the Nissen?
For most patients, yes. Meta-analyses of randomised trials show no significant difference in heartburn, regurgitation, or acid exposure between the two, despite the Nissen producing a marginally higher valve pressure.
Why does the Nissen cause more side effects?
Because a full 360° wrap creates a tighter barrier. That makes it harder for food to pass when swallowing (dysphagia) and harder for gas to escape when belching (gas-bloat). The Toupet’s partial wrap leaves more room, so these problems are less common.
Which is better if I have weak oesophageal motility?
Traditionally a partial wrap like the Toupet was recommended for weak motility, but a randomised trial found the Toupet’s lower dysphagia applied regardless of motility, questioning that rule. Practice still varies, so this is a decision for your surgeon based on your specific tests.
Can I still belch and vomit after these operations?
It is generally easier after a Toupet than a Nissen, because the partial wrap leaves more room for gas to escape. A full Nissen wrap more often causes trapped gas and difficulty belching, though this frequently eases over time.
How long do the results last?
Both are durable operations with good long-term outcomes, and pooled data show comparable reflux control over the long term. As with any surgery, results depend on patient selection, technique, and the experience of the surgeon.
Research Sources
- [Du et al., BMC Gastroenterology, 2016] — A meta-analysis of eight randomised trials found no significant difference between Nissen and Toupet in heartburn, regurgitation, acid exposure, or oesophagitis, but higher rates of dysphagia, gas-bloat, inability to belch, dilatation, and reoperation after Nissen.
- [Tian et al., PLoS One, 2015] — A meta-analysis of 13 randomised trials found the two operations equally effective at controlling reflux, but with significantly more dysphagia, gas-bloat, inability to belch, and reoperation after the full Nissen wrap.
- [Booth et al., British Journal of Surgery, 2008] — A randomised trial stratified by oesophageal motility found dysphagia and chest pain on eating were significantly more common after Nissen, with no difference between motility groups, concluding there was no need to tailor the wrap to preoperative manometry.
- [Strate et al., Surgical Endoscopy, 2008] — A randomised trial of 200 patients evaluating the tailored concept, comparing Nissen and Toupet outcomes in patients with and without oesophageal motility disorders.
David Gray
Content Researcher & Author
David Gray founded Wipeout Reflux to address a critical gap in reflux management. His research synthesizes over 100 peer-reviewed studies on laryngopharyngeal reflux (LPR), pepsin biology, and GERD pathophysiology. For LPR specifically—a condition most physicians misdiagnose—his work focuses on pepsin reactivation and why standard PPI therapy fails most patients. He develops evidence-based protocols targeting root causes of both LPR and GERD, integrating emerging research on sphincter dysfunction, dietary interventions, and newer clinical approaches. Wipeout Reflux represents practical application of clinical science for patients seeking real solutions.