
One question puzzled me for years with silent reflux: why is the throat so much more delicate than the food pipe below it? People with ordinary heartburn can have acid splashing their oesophagus (the tube that carries food to the stomach) for years before it causes real trouble. Yet a tiny amount of reflux reaching the throat can leave it raw, hoarse and sore. Why the difference?
The answer is something called mucosal defence — the throat’s built-in protection against acid — and one little helper in particular that hardly anyone talks about: an enzyme called carbonic anhydrase.
Here’s the simple version. Your throat protects itself from acid by making its own acid-neutraliser on the spot, and carbonic anhydrase is the tool it uses to do that. The cruel catch is that pepsin — a stomach enzyme carried up in reflux — quietly breaks that tool. So reflux doesn’t just irritate your throat; it dismantles the very defence that’s meant to protect it. That’s a huge part of why laryngopharyngeal reflux (LPR), or silent reflux, can be so stubborn.
This is one of the most important ideas in LPR, and once it clicks, a lot of things make sense. Let me walk you through it in plain English.
Key takeaways
- Mucosal defence is your throat’s built-in protection against stomach acid and pepsin.
- Your throat has much weaker defences than your food pipe, which is why it’s more easily damaged by reflux.
- Your food pipe can pour out a protective “acid-neutraliser” (bicarbonate); your throat can’t do this the same way.
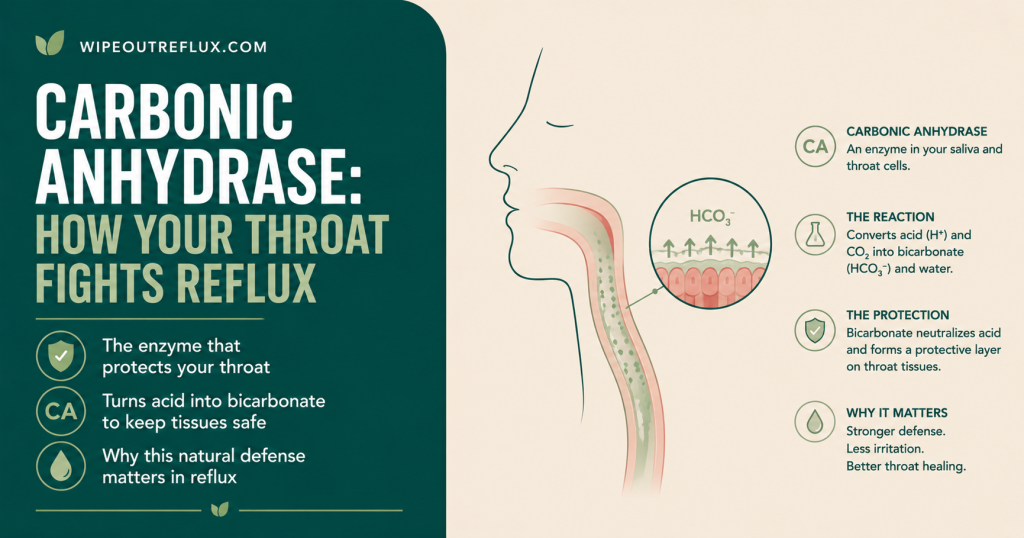
- Instead, the throat relies on an enzyme called carbonic anhydrase III (CAIII) to make bicarbonate inside its cells to cancel out acid.
- Repeated exposure to pepsin uses up this enzyme, so the throat slowly loses its ability to neutralise acid.
- Pepsin also weakens the “glue” holding throat cells together, making the lining leakier.
- This becomes a cycle: reflux brings pepsin, pepsin wears down the defences, and the weakened throat copes even worse with the next reflux.
- Because the throat’s own acid-neutraliser runs low, getting bicarbonate from other sources — like saliva and diet — becomes really important.
What “mucosal defence” actually means
Think of your throat and food pipe as having a protective shield against the acid and enzymes that reflux can bring up. That shield is what doctors call mucosal defence, and it works in layers, a bit like the defences of a well-built house.
The outer layer is a thin coating of mucus and bicarbonate on the surface — like a protective film — topped up by the saliva you swallow. It soaks up acid before it can reach the cells underneath. The middle layer is the wall of cells themselves, packed tightly together so acid can’t slip between them, with their own internal kit for neutralising any acid that gets through. The inner layer is the blood supply beneath, which carries acid away.
When this shield is intact, refluxed acid gets soaked up and pushed back. When it breaks down, acid and pepsin reach the tissue and cause damage. And here’s the key point: your throat’s shield is far flimsier than your food pipe’s.
Why your throat is so much more fragile than your food pipe
This is really the heart of it. Your oesophagus has special glands in its wall that actively pump out bicarbonate — nature’s antacid — creating a proper protective blanket around its cells. Your throat has no such glands. It simply can’t pour out bicarbonate the way the food pipe can.
Instead, the throat has to make bicarbonate inside its own cells, using a little tool called carbonic anhydrase. That’s a much thinner, more easily overwhelmed line of defence. It’s the difference between a house with thick walls and one with thin ones — the same storm that the thick-walled house shrugs off can flood the thin-walled one. That’s exactly why the same reflux an oesophagus might tolerate can leave a throat inflamed, and it’s central to how I explain the difference in my GERD vs LPR comparison.
What carbonic anhydrase actually does
Carbonic anhydrase III (CAIII for short) is the version of this enzyme found in the throat lining. Its job is simple and clever: it helps the cells make bicarbonate — that natural acid-neutraliser — right where it’s needed. When acid arrives, the bicarbonate cancels it out and nudges things back to a safe balance.
In a healthy throat, this little enzyme is quietly at work, mopping up the small acid challenges that come its way. In other words, it’s the throat’s own on-site antacid factory. When it’s running, it does a genuinely good job. The problems start when reflux shuts that factory down.
How pepsin breaks the throat’s defences
Here’s where it all connects. When reflux reaches your throat, it leaves behind pepsin — an enzyme from the stomach — in the tissue. And repeated exposure to pepsin uses up carbonic anhydrase III, along with another protective protein the throat relies on [Johnston et al., The Laryngoscope, 2007].
This isn’t just a theory — it shows up in real patients. In tiny throat tissue samples, pepsin was found in 8 out of 9 people with LPR, but in none of 12 healthy people. And where pepsin was present, carbonic anhydrase III was noticeably depleted [Johnston et al., The Laryngoscope, 2004]. A larger follow-up study found the same thing: in people with LPR, carbonic anhydrase III was missing from much of the throat lining, and the “glue” that holds throat cells tightly together — a protein called E-cadherin — was reduced too [Gill et al., Annals of Otology, Rhinology & Laryngology, 2005].
So pepsin does two kinds of harm at once. It shuts down the throat’s antacid factory, so the tissue can’t neutralise acid as well. And it loosens the glue between cells, so the lining becomes leakier and acid and pepsin can sink in deeper. Your throat’s chemical defence and its physical barrier both take a hit at the same time.
The cycle that keeps it going
Put those pieces together and you can see why silent reflux is so persistent. Reflux brings pepsin to the throat. Pepsin wears down the carbonic anhydrase, so the throat makes less bicarbonate. With less bicarbonate, the throat can’t keep its acid levels in check — and that matters a lot, because pepsin sitting in the tissue springs back to life whenever things turn acidic, something I explain in my guide to neutralising pepsin in the throat. That reawakened pepsin causes more damage and wears down even more of the defence. Round and round it goes, with the throat a little more exposed each time.
That’s the honest reason silent reflux tends to build rather than simply fade on its own — and why just removing the acid often isn’t enough, because the defences themselves have been chipped away. If you’d like the full background on the enzyme at the centre of all this, my explainer on what pepsin is ties it together.
Why this matters for treatment
Understanding mucosal defence changes how you think about tackling LPR.
First, it explains why acid-blocking tablets so often disappoint. Proton pump inhibitors (PPIs) turn down how much acid your stomach makes, but they don’t remove pepsin that’s already lodged in your throat, and they don’t rebuild the depleted carbonic anhydrase. That’s part of why up to 40% of people with LPR don’t get enough relief from PPIs alone. I dig into this in my guide on coming off PPIs and acid rebound.
Second, it points to what actually helps. You can’t simply top up carbonic anhydrase with a pill, so the goal is to protect the defences you’ve still got. That means three things: cutting down how much pepsin reaches your throat in the first place by reducing reflux; keeping your throat calm and low in acid so any lodged pepsin stays asleep instead of causing fresh damage; and — since your throat is short on its own acid-neutraliser — bringing in bicarbonate from outside. That’s exactly why saliva matters so much here. Chewing sugar-free gum boosts saliva, which delivers extra bicarbonate to help out, as I cover in my guide to chewing gum for acid reflux — and it’s also why some people find alkaline water a handy buffering tool.
One honest note: this is about understanding the mechanism so you can protect your throat sensibly — it’s not a switch you can simply flick back on. Carbonic anhydrase and pepsin are being studied as possible ways to diagnose LPR, but that’s still research rather than an everyday test. What you can do is give your throat less to deal with and more time to heal.
Conclusion
Mucosal defence is the missing piece that explains why silent reflux hits the throat so hard. Your throat never had the strong acid defences your food pipe enjoys — it leans instead on carbonic anhydrase to make its own protection from within. When pepsin arrives with reflux and wears that enzyme down, while also loosening the glue between cells, the throat is left doubly exposed, and every reflux episode chips away at its ability to handle the next. It’s a quiet, self-feeding wearing-down of your defences, and it’s why LPR so rarely just clears up by itself.
But there’s real hope in understanding it. If reflux is what’s wearing down your throat’s defences, then protecting those defences becomes the whole game: fewer reflux episodes so less pepsin arrives, a calmer and less acidic throat so any lodged pepsin stays asleep, and bicarbonate from saliva and diet to stand in for the protection your throat struggles to make. None of it needs a miracle — just a steady, sensible approach.
That’s exactly what my Wipeout Diet Plan is designed to deliver — a clear, step-by-step programme built to reduce the pepsin and acid reaching your throat, so your remaining defences aren’t constantly under siege. It goes far deeper into the how and why than any single article can. And to make everyday choices easy, the Wipeout Food Reference Guide is the essential companion, laying out the foods and drinks allowed on an acid reflux and LPR diet along with their pH values — so you can keep your throat calm enough for its defences to hold and heal. Together they turn the science on this page into a plan you can genuinely live by.
Frequently asked questions
What is mucosal defence in the throat?
Mucosal defence is your throat’s built-in protection against acid and pepsin. It works in layers: a surface film of mucus and bicarbonate, cells packed tightly together, an internal acid-neutralising system, and the blood supply beneath. When these defences hold, refluxed acid is soaked up and pushed back; when they break down, the throat gets damaged.
What does carbonic anhydrase do in the throat?
Carbonic anhydrase III (CAIII) is an enzyme in the throat lining that helps the cells make bicarbonate — a natural acid-neutraliser — right where it’s needed. That bicarbonate cancels out refluxed acid and keeps things balanced. It’s especially important in the throat because, unlike the food pipe, the throat can’t pour bicarbonate out from glands.
Why is the throat more easily damaged by reflux than the food pipe?
The oesophagus (food pipe) has glands that actively release bicarbonate to form a protective blanket around its cells. The throat has no such glands and instead relies on carbonic anhydrase working inside its cells — a thinner, more easily overwhelmed defence. That’s why a small amount of reflux reaching the throat can cause more trouble than years of acid in the food pipe.
How does pepsin damage the throat’s defences?
Pepsin left behind in the throat during reflux uses up carbonic anhydrase III, so the tissue can no longer make enough bicarbonate to neutralise acid. It also reduces E-cadherin, the “glue” holding throat cells tightly together, making the lining leakier. Studies of throat tissue confirm both the presence of pepsin and the loss of these protective proteins in people with LPR.
Can carbonic anhydrase be restored once it’s used up?
There’s no supplement or drug that reliably rebuilds it. The practical approach is to protect what you have rather than try to replace it: reduce how much pepsin reaches the throat, keep things low in acid so lodged pepsin stays asleep, and give the tissue time to recover. Bringing in bicarbonate from saliva and diet helps make up for the shortfall.
Why don’t acid-blocking tablets fix this?
Proton pump inhibitors (PPIs) reduce stomach acid, but they don’t remove pepsin already sitting in your throat, and they don’t rebuild the depleted carbonic anhydrase or repair the weakened barrier. That’s a big reason up to 40% of people with LPR don’t get enough relief from PPIs alone, and why a broader, defence-protecting approach tends to work better.
How can I protect my throat’s defences?
Focus on reducing reflux so less pepsin reaches the throat, keeping your diet low in acid so lodged pepsin isn’t reawakened, and bringing in bicarbonate from outside — boosting saliva with sugar-free gum and considering alkaline water. Because your throat’s own bicarbonate supply runs low in LPR, these outside sources become especially valuable.
Research sources
- [Johnston et al., The Laryngoscope, 2004] — Pepsin was found in 8 of 9 people with LPR and none of 12 healthy people, and where pepsin was present, carbonic anhydrase III was depleted in the throat lining, leaving it more open to reflux damage.
- [Gill et al., Annals of Otology, Rhinology & Laryngology, 2005] — In throat tissue samples from people with LPR, pepsin was present, carbonic anhydrase III was missing from much of the lining, and the cell-to-cell “glue” E-cadherin was reduced, pointing to a weakened barrier.
- [Johnston et al., The Laryngoscope, 2007] — Showed that exposing the throat lining to pepsin uses up its protective proteins, including carbonic anhydrase III, and explained how pepsin’s activity depends on acidity.
David Gray
Content Researcher & Author
David Gray founded Wipeout Reflux to address a critical gap in reflux management. His research synthesizes over 100 peer-reviewed studies on laryngopharyngeal reflux (LPR), pepsin biology, and GERD pathophysiology. For LPR specifically—a condition most physicians misdiagnose—his work focuses on pepsin reactivation and why standard PPI therapy fails most patients. He develops evidence-based protocols targeting root causes of both LPR and GERD, integrating emerging research on sphincter dysfunction, dietary interventions, and newer clinical approaches. Wipeout Reflux represents practical application of clinical science for patients seeking real solutions.