
Most reflux advice fixates on the valve at the top of the stomach — and it matters. But there is a second half of the story that gets almost no attention: how quickly your esophagus cleans up after acid comes back up. That job belongs to esophageal motility, the coordinated muscular wave that normally sweeps refluxed acid back down where it belongs.
Here is the short version. When motility is strong, refluxed acid is cleared in seconds and does little harm. When motility is weak or disordered — a condition called ineffective esophageal motility — that acid lingers on the lining far longer, causing more damage, more symptoms, and, for silent reflux, a greater chance of the refluxate reaching your throat. In other words, reflux disease isn’t only about how much acid escapes; it’s also about how fast you clean it up.
Let me walk through how esophageal motility works, what happens when it fails, and why it matters so much for silent reflux in particular.
Key takeaways
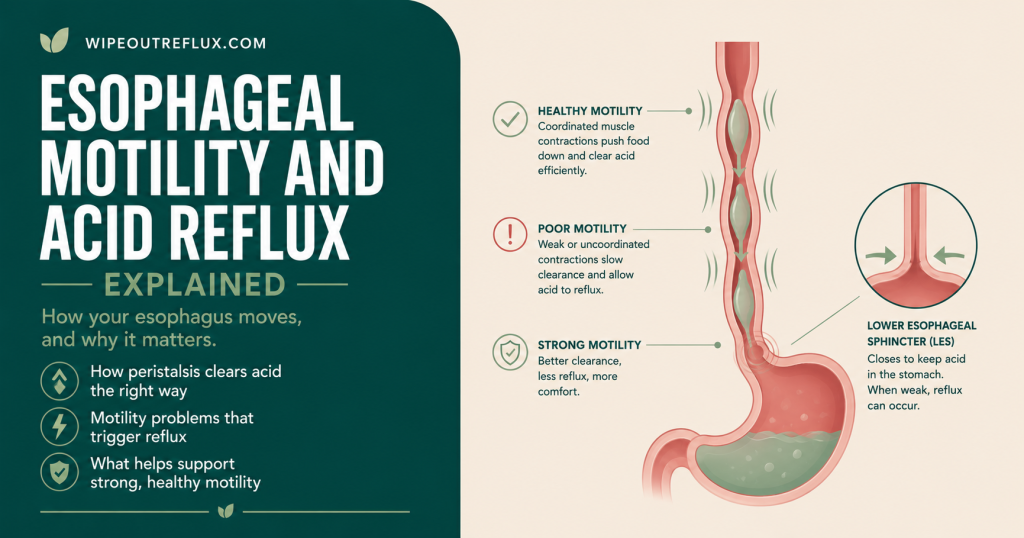
- Esophageal motility is the coordinated wave of muscle contraction (peristalsis) that moves food down and sweeps refluxed acid back into the stomach.
- Acid clearance happens in two steps: peristalsis clears the bulk of the acid, then swallowed saliva neutralises what’s left.
- Ineffective esophageal motility (IEM) means weak or failed contractions that don’t clear acid efficiently.
- Poor motility leaves acid in contact with the lining longer, causing more damage and more severe symptoms.
- Around a fifth of people with reflux disease have significantly impaired peristalsis, and this group tends to have worse reflux.
- Reflux and poor motility can feed each other — acid damage can impair the muscle, which then clears acid even less well.
- For silent reflux, slower clearance means refluxate is more likely to climb high enough to reach the throat.
- Acid-suppressing drugs don’t improve motility, so reducing reflux and using gravity and saliva to help clearance become key.
What esophageal motility actually is
Your esophagus isn’t a passive tube. It’s a muscular one, and it moves things along with peristalsis — a wave of coordinated contraction that travels from your throat down to the stomach, squeezing contents ahead of it.
There are two kinds worth knowing. Primary peristalsis is the wave triggered every time you swallow, carrying food and drink down. Secondary peristalsis is the automatic one: a wave triggered by something stretching or irritating the esophagus — such as refluxed acid — without you needing to swallow. That secondary wave is essentially your esophagus’s built-in cleanup reflex, and it is central to protecting you from reflux.
How motility clears acid: the two-step system
When acid refluxes into your esophagus, it’s cleared in two sequential stages, and motility drives the first one.
Step one — volume clearance. One or two peristaltic waves rapidly sweep almost all of the refluxed liquid back down into the stomach. This is the heavy lifting, and it’s done by muscle. Step two — chemical clearance. That leaves behind a thin residue that keeps the pH low, and swallowed saliva then neutralises it with bicarbonate, restoring a safe pH [Helm et al., New England Journal of Medicine, 1984].
The two work as a team: peristalsis removes the bulk, saliva mops up the rest. If either step falters, acid sits on the lining longer. I’ve written separately about the saliva side of this in my guide to chewing gum and acid reflux, since stimulating saliva is one way to boost that second stage. This article is about the first stage — the muscle.
When motility fails: ineffective esophageal motility
Ineffective esophageal motility, or IEM, is the most common motility problem seen in reflux disease. It means a large proportion of the peristaltic contractions are too weak (below about 30 mmHg) or simply fail to travel the full length of the esophagus. When the wave is weak, it can’t do its job of sweeping acid back down.
The consequences are exactly what you’d predict. In a large study of people with reflux disease, esophageal peristalsis was severely impaired in around 21% of patients — and that group had more severe reflux, slower acid clearance, worse damage to the lining, and more severe respiratory symptoms than those with normal motility [Diener et al., Journal of Gastrointestinal Surgery, 2001]. The weaker the wave, the longer acid stays in contact with the tissue, and the more harm it does.
The vicious circle of reflux and poor motility
Here’s a detail that makes reflux so stubborn once it’s established: the relationship between acid and motility runs both ways. Reflux damages the esophageal lining, and that damage can in turn impair the muscle’s ability to contract properly. Weaker contractions then clear acid less effectively, which means more acid exposure, which causes more damage. Fittingly, studies have found that peristaltic dysfunction becomes more common and more severe as esophagitis worsens [Kahrilas et al., Gastroenterology, 1986]. Reflux and poor motility can quietly reinforce each other.
Why motility matters even more for silent reflux
This is where esophageal motility connects directly to laryngopharyngeal reflux (LPR). Think of it alongside the valves: even when reflux gets past the lower valve, strong motility limits how long the acid stays and how far up it travels. Weak motility does the opposite — the refluxate lingers, and lingering refluxate is far more likely to climb high enough to reach the upper esophagus and spill into the throat.
That’s not just theory. Impaired motility is strongly linked to the extra-esophageal, respiratory-type symptoms that characterise silent reflux, and the study above found respiratory symptoms were more severe in those with ineffective motility. It fits the wider picture I describe in my GERD vs LPR comparison and my overview of LPR symptoms: the longer acid and pepsin linger, the more chance they have to reach and reactivate in your throat, a process I unpack in my guide to neutralising pepsin in the throat.
What affects your esophageal motility
Some influences on motility you can act on, and some you can’t. Reflux itself is a major one, through the mucosal-damage loop described above. Age also plays a role — peristalsis tends to weaken as we get older. Certain systemic conditions, particularly connective tissue disorders like scleroderma, can severely impair esophageal muscle, and some medications affect motility too.
The honest reality is that motility is partly structural and physiological, not something you can fully control the way you can control meal timing or trigger foods. That doesn’t make you powerless — it just shifts where the useful effort goes.
What actually helps when motility is the issue
If clearance is slow, the goal is to give your esophagus less to clear and to help it clear what remains.
Reduce reflux events in the first place
The less acid that comes up, the less your motility has to deal with. That means the core anti-reflux habits: smaller and earlier meals, managing weight around the middle, and protecting the valve, which I cover in my guide to the stomach sphincter and LPR.
Let gravity do the work motility can’t
When peristalsis is weak, gravity becomes your best ally. Stay upright for a few hours after eating, elevate the head of your bed, and sleep on your left side — all of which help refluxed material drain back down without relying on a strong muscular wave. My guides to night-time reflux and the best sleeping position for silent reflux go into this.
Boost the second stage of clearance
Since saliva handles chemical clearance, stimulating it — chewing sugar-free, non-mint gum after meals, staying hydrated — helps compensate when the muscular stage is underperforming.
Know the limits of medication
This is important: acid-suppressing drugs reduce the acidity of what you reflux, but they do not improve esophageal motility. For diagnosed dysmotility with persistent symptoms, specialists sometimes use prokinetic medications, and high-resolution manometry is the test that actually diagnoses motility problems. Those are conversations to have with a gastroenterologist rather than steps to self-prescribe.
Conclusion
Esophageal motility is the unsung half of reflux. The valves get all the attention, but how quickly your esophagus clears acid afterwards is just as important to whether that acid causes damage. Strong peristalsis sweeps refluxate away in seconds; weak or ineffective motility lets it linger, deepening the injury and, in silent reflux, giving acid and pepsin the time they need to climb up and reach your throat. And because reflux and poor motility can reinforce each other, it’s a cycle well worth interrupting early.
The empowering part is that even when motility itself is hard to change, the things that matter most are firmly in your hands. Give your esophagus less to clear by reducing reflux at the source, lean on gravity when the muscle can’t do it all, and support the saliva side of clearance. Together, these take real pressure off a system that may not be working at full strength.
That source-first approach is exactly what my Wipeout Diet Plan is built around — a structured, step-by-step programme for calming reflux so your esophagus has far less to clear in the first place, going deeper into the mechanisms and the daily routine than any single article can. And to make everyday choices simple, the Wipeout Food Reference Guide is the essential companion, laying out the foods and drinks allowed on an acid reflux and LPR diet along with their pH values — so you can build meals that trigger less reflux and less acid for your motility to cope with. Together they turn the science on this page into a plan you can genuinely live by.
Frequently asked questions
What is esophageal motility?
Esophageal motility is the coordinated muscular movement — peristalsis — that pushes food and drink down your esophagus into the stomach and sweeps refluxed acid back down. Primary peristalsis is triggered by swallowing, while secondary peristalsis is an automatic wave triggered by reflux or stretching, acting as your esophagus’s built-in cleanup reflex.
How does esophageal motility affect acid reflux?
Motility drives acid clearance. When refluxed acid enters the esophagus, peristaltic waves sweep the bulk of it back down, and saliva neutralises the rest. Strong motility clears acid in seconds; weak motility lets it sit on the lining much longer, causing more damage and more severe symptoms. So reflux disease is partly about how efficiently you clear acid, not just how much escapes.
What is ineffective esophageal motility (IEM)?
IEM is the most common motility abnormality in reflux disease. It means a large share of the peristaltic contractions are too weak or fail to travel the full length of the esophagus, so acid isn’t cleared efficiently. People with IEM tend to have longer acid exposure, slower clearance, and more severe reflux and mucosal damage than those with normal motility.
Can acid reflux cause poor esophageal motility?
It can contribute to it. Reflux damages the esophageal lining, and that damage can impair the muscle’s ability to contract effectively. Weaker contractions then clear acid less well, allowing more exposure and more damage — a self-reinforcing cycle. This is one reason established reflux can become harder to control over time, and why acting early helps.
Does esophageal motility matter for silent reflux?
Yes, significantly. Weak motility means refluxate lingers longer and is more likely to climb high enough to reach the throat, which is exactly what happens in silent reflux (LPR). Impaired motility is closely linked to the respiratory and throat-based symptoms that characterise LPR, making efficient clearance an important part of the picture.
Can you improve esophageal motility?
Motility is partly structural, so you can’t reliably “train” it stronger with a food or exercise. What you can do is reduce how much reflux it has to clear, use gravity by staying upright and elevating the head at night, and support saliva-based clearance. For diagnosed dysmotility with ongoing symptoms, a gastroenterologist may consider prokinetic medication.
How is esophageal motility tested?
The main test is high-resolution manometry, which measures the strength and coordination of the peristaltic waves along your esophagus using a thin catheter. It’s the tool that diagnoses ineffective esophageal motility and other motility disorders, and it’s usually arranged by a gastroenterologist when clearance problems are suspected.
Research sources
- [Diener et al., Journal of Gastrointestinal Surgery, 2001] — In 1,006 patients with reflux disease, severely impaired peristalsis (IEM) was present in about 21%, and this group had more severe reflux, slower acid clearance, worse mucosal injury, and more severe respiratory symptoms.
- [Helm et al., New England Journal of Medicine, 1984] — Established the two-step model of esophageal acid clearance: peristalsis rapidly clears the volume of refluxate, after which swallowed saliva neutralises the residual acid.
- [Kahrilas et al., Gastroenterology, 1986] — Found that esophageal peristaltic dysfunction becomes progressively more common and severe with increasing severity of reflux esophagitis, supporting a link between mucosal damage and impaired motility.
David Gray
Content Researcher & Author
David Gray founded Wipeout Reflux to address a critical gap in reflux management. His research synthesizes over 100 peer-reviewed studies on laryngopharyngeal reflux (LPR), pepsin biology, and GERD pathophysiology. For LPR specifically—a condition most physicians misdiagnose—his work focuses on pepsin reactivation and why standard PPI therapy fails most patients. He develops evidence-based protocols targeting root causes of both LPR and GERD, integrating emerging research on sphincter dysfunction, dietary interventions, and newer clinical approaches. Wipeout Reflux represents practical application of clinical science for patients seeking real solutions.