
If you have reflux, almost everything traces back to one small ring of muscle: the lower esophageal sphincter, or LES. It is the valve sitting between your esophagus and your stomach, and when it does its job, you never think about it. When it does not, you get heartburn, regurgitation, or — in my case for years — the throat and voice symptoms of silent reflux.
I get asked about the LES constantly, usually phrased as “what actually causes reflux in the first place?” So this is the plain-English explainer I wish I’d had years ago: what the LES is, how it works, the three ways it fails, and why it matters even more if your reflux is the silent, throat-based kind.
Key takeaways
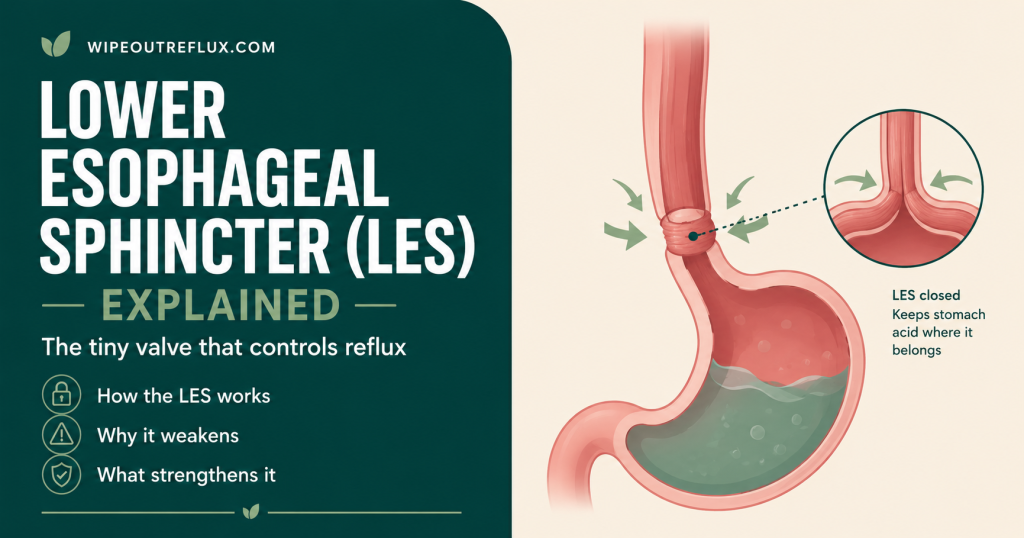
- The lower esophageal sphincter (LES) is a ring of muscle at the junction of the esophagus and stomach that acts as a one-way valve.
- At rest it stays tightly closed, holding a pressure higher than the stomach so acid and pepsin cannot flow back up.
- It relaxes for a few seconds when you swallow, then closes again — that timing is the whole game.
- Reflux happens when the LES fails in one of three ways: transient relaxations, weak resting tone, or an anatomical problem like a hiatal hernia.
- Transient LES relaxations (TLESRs) — brief, unprompted openings triggered by a stretched stomach — are the single most common cause of reflux.
- For silent reflux (LPR), the LES is only the first gate; the refluxate must also breach the upper esophageal sphincter to reach your throat.
- You cannot “tighten” the LES with a food or supplement, but you can dramatically reduce how often it is challenged.
- Large meals, late eating, excess weight around the middle, and certain foods and drinks all work by provoking the LES.
What is the lower esophageal sphincter?
The LES is a specialised band of circular smooth muscle, roughly 3 to 4 cm long, wrapped around the bottom end of your esophagus where it meets the stomach. This junction is called the esophagogastric junction, and it is one of the most important pieces of anti-reflux plumbing in your body.
Unlike a valve you might picture from a diagram, the LES is not a simple flap. It is actually a partnership between two structures: the intrinsic muscle of the sphincter itself, and the crural diaphragm — the part of your breathing muscle that wraps around the esophagus and acts as an external clamp. Together they form a high-pressure zone that resists the constant upward push from the stomach [Manzo et al., Annals of Laparoscopic and Endoscopic Surgery, 2021]. That partnership matters, and it is exactly what a hiatal hernia disrupts — more on that shortly.
If you want the wider context of how this valve fits into silent reflux specifically, I cover it in my guide to the stomach sphincter and LPR.
How the LES works
Think of the LES as a gate that is closed by default. At rest it holds a tone roughly 10 to 30 mmHg above the pressure inside your stomach. That pressure difference is the barrier — as long as the gate holds more pressure than the stomach beneath it, nothing comes back up.
When you swallow, nerves signal the LES to relax for about 5 to 7 seconds, letting the food or liquid pass into the stomach, and then it snaps shut again. It also opens deliberately during a belch, to vent gas. The control is neural: your vagus nerve drives the timing, with nitric oxide signalling relaxation and acetylcholine helping maintain the squeeze.
So the healthy pattern is simple — closed, brief opening to swallow, closed again. Reflux is what happens when that pattern breaks down.
The three ways the LES fails
This is the part worth understanding properly, because “weak valve” is the lazy explanation you see everywhere, and it is only one of three mechanisms — and not even the most common one.
1. Transient LES relaxations (the big one)
A transient LES relaxation, or TLESR, is when the sphincter suddenly relaxes on its own, without a swallow to justify it, and stays open longer than a normal swallow-relaxation would. These unprompted openings are the most frequent cause of reflux in both healthy people and people with reflux disease [Bentley et al., Physiological Reports, 2024].
Here is the key trigger: TLESRs are set off mainly by a stretched stomach. When the stomach is distended by a large meal, by swallowed air, or by the gas from fizzy drinks, a reflex fires that relaxes the LES — essentially the belch reflex, letting pressure escape. The problem is that when it opens, acid and pepsin can slip up with the gas.
This single mechanism explains why so much practical advice works. Smaller meals, not overfilling your stomach, going easy on carbonation, and not swallowing lots of air all reduce gastric distension, which reduces how often these relaxations fire. You are not “strengthening” anything — you are removing the trigger.
2. Low resting LES pressure (a genuinely weak valve)
In some people the baseline tone of the LES is simply too low, so the gate never holds enough pressure to reliably keep the stomach’s contents down. This tends to show up in more severe reflux, and the degree of weakness often tracks with the severity of damage to the esophagus. Interestingly, there is evidence that repeated acid exposure can itself weaken the sphincter over time, which sets up a vicious circle — reflux weakens the LES, and a weaker LES allows more reflux.
3. Hiatal hernia and anatomical disruption
Remember that the LES works in partnership with the crural diaphragm. Normally the two sit at the same level, stacked on top of each other for a double seal. A hiatal hernia is when part of the stomach slides up through the diaphragm, pulling the LES away from its diaphragmatic backup. The two anti-reflux components separate, the high-pressure zone weakens, and reflux becomes much easier — especially when abdominal pressure rises [Manzo et al., Annals of Laparoscopic and Endoscopic Surgery, 2021].
The LES and silent reflux (why it’s only the first gate)
Here is where silent reflux, or laryngopharyngeal reflux (LPR), differs from ordinary heartburn, and where a lot of generic content falls short.
For refluxate to reach your throat and voice box, it has to get past two valves, not one: the LES at the bottom of the esophagus, and the upper esophageal sphincter (UES) at the top. In fact, the body has four defences against reflux reaching the larynx — the LES, the UES, the wave-like clearing action of the esophagus, and the tissue’s own resistance [Laryngopharyngeal Reflux, StatPearls, 2025].
So in classic GERD, a failing LES lets acid into the esophagus and you feel heartburn. In LPR, the refluxate not only gets past the LES but also breaches the UES, reaching the far more delicate tissues of the throat — where even small, brief exposures cause symptoms. Research backs this up: weaker upper-sphincter function correlates with more severe LPR symptoms [Wu et al., Scientific Reports, 2021].
The practical upshot is important. The LES is still your first line of defence, so protecting it helps everyone. But if you have silent reflux, addressing the LES alone may not be the full story — which is a big reason LPR can be so stubborn. I unpack the differences fully in my GERD vs LPR comparison, and the wider symptom picture in my rundown of LPR symptoms.
What weakens or relaxes the LES
Plenty of everyday things nudge the LES in the wrong direction, either by lowering its resting tone or by triggering those transient relaxations. The common ones:
- Large meals — the biggest lever, because they distend the stomach and drive TLESRs.
- Lying down after eating — removes gravity’s help while the stomach is still full. This is why night-time reflux is so common.
- Excess weight around the midsection — raises intra-abdominal pressure, pushing against the LES.
- High-fat meals — slow stomach emptying, keeping it distended longer.
- Certain foods and drinks — chocolate, peppermint, caffeine and alcohol are all classically associated with reduced LES tone.
- Smoking — lowers sphincter pressure and reduces saliva that would otherwise help clear acid.
- Some medications — a number of common drugs can relax the LES; worth reviewing with your doctor rather than stopping anything yourself.
- Pregnancy — hormonal changes plus rising abdominal pressure both play a role.
Can you strengthen or fix the LES?
I want to be honest here, because this is where a lot of misleading claims live. There is no food, drink or supplement that “tightens” the LES in any meaningful, lasting way. If you see that promise, be sceptical.
What you can do is reduce how often the LES is challenged, so it does not need to be a perfect valve to keep you comfortable. That means smaller and earlier meals, keeping weight around the middle in check, easing off your personal trigger foods, and staying upright after eating. These measures work by lowering gastric distension and abdominal pressure — the very things that provoke the sphincter.
Two more practical points. First, an alginate such as Gaviscon Advance forms a physical raft on top of the stomach contents, which helps compensate when the LES does open — a genuinely useful tool rather than a cure. Second, some people explore diaphragm-focused training like the IQoro device, working on the crural diaphragm side of that anti-reflux partnership.
For severe, well-documented cases where the valve genuinely fails, there are procedures that target the LES directly — from the Stretta procedure to surgical options I cover in my guide to LPR surgery. These are decisions to make with a specialist, not first steps.
Frequently asked questions
What does the lower esophageal sphincter do?
It acts as a one-way valve between your esophagus and stomach. At rest it stays closed, holding a pressure higher than the stomach so acid and pepsin cannot travel back up. It relaxes briefly when you swallow to let food and liquid pass, then closes again. This on-off timing is what prevents reflux.
What causes the LES to weaken or open when it shouldn’t?
The most common cause is a transient LES relaxation — an unprompted opening triggered mainly by a stretched stomach from large meals, swallowed air or fizzy drinks. Other causes include genuinely low resting muscle tone and anatomical problems like a hiatal hernia. Certain foods, excess abdominal weight, smoking and some medications also reduce LES tone.
Is the LES the only thing that stops silent reflux?
No, and this is central to understanding LPR. Your throat is protected by two valves — the lower esophageal sphincter and the upper esophageal sphincter — plus the esophagus’s clearing action and the tissue’s own resistance. Silent reflux involves the refluxate getting past both sphincters to reach the throat, which is why it can persist even when heartburn is absent.
Can you strengthen the lower esophageal sphincter naturally?
Not in the sense of tightening the muscle with a food or supplement — that is a myth. What genuinely helps is reducing how often the sphincter is challenged: smaller and earlier meals, managing weight around the middle, avoiding trigger foods and staying upright after eating. These lower the gastric distension and abdominal pressure that provoke the LES in the first place.
How is a hiatal hernia connected to the LES?
Normally the LES sits level with the crural diaphragm, and the two form a double seal. A hiatal hernia occurs when part of the stomach slides up through the diaphragm, separating the LES from its diaphragmatic support. This weakens the combined high-pressure zone and makes reflux easier, particularly when abdominal pressure rises.
Does a weak LES always mean you’ll have reflux?
Not necessarily. Many people with mild reflux have normal resting LES tone, with their reflux driven mainly by transient relaxations rather than a permanently weak valve. Equally, some people with a hiatal hernia have little or no reflux because their remaining defences compensate. The LES is the biggest single factor, but reflux is the result of the whole system.
Can medication tighten the LES?
Standard reflux medications like PPIs and H2 blockers reduce stomach acid; they do not tighten the LES. There are drug classes studied for reducing transient LES relaxations, but they are not in routine use for most people. In practice, lifestyle measures plus an alginate to compensate physically are the mainstays for supporting a leaky valve.
Conclusion
The lower esophageal sphincter is the quiet gatekeeper behind almost every reflux symptom. Understanding it changes how you approach the problem: instead of chasing symptoms, you start asking what is provoking the valve — and the answer is usually a stretched stomach from large or late meals, extra abdominal pressure, or specific trigger foods. Those transient relaxations, not a permanently broken valve, are what most people are actually dealing with, and that is genuinely good news, because they respond to how and when you eat.
For silent reflux there is an extra layer: the refluxate has to breach two sphincters to reach your throat, which is exactly why LPR can feel so persistent and why protecting the LES, while essential, is only part of the plan. The most reliable path is to reduce the demands on the valve consistently, day after day, rather than hunting for a food that magically tightens it.
That is the whole philosophy behind my Wipeout Diet Plan — a structured, step-by-step programme for calming reflux at the source and giving your sphincters far less to cope with, covering the mechanisms and the practical routine in real depth. And if you simply want to know which foods and drinks are safe to build meals around, the Wipeout Food Reference Guide is the essential quick-reference companion, laying out the foods and drinks allowed on an acid reflux and LPR diet along with their pH values. Together they give you both the deeper roadmap and the everyday cheat sheet to keep that gatekeeper on your side.
Research sources
- [Bentley et al., Physiological Reports, 2024] — Describes the LES as a tonically contracted smooth-muscle anti-reflux barrier and notes the strong association between frequent transient LES relaxations and GERD.
- [Manzo et al., Annals of Laparoscopic and Endoscopic Surgery, 2021] — Reviews the esophagogastric junction as a dual barrier formed by the intrinsic LES and the crural diaphragm, and how hiatal hernia separates them and weakens the anti-reflux barrier.
- [Laryngopharyngeal Reflux, StatPearls, 2025] — Outlines the four barriers protecting the larynx from reflux: the LES, the UES, esophageal peristalsis, and epithelial resistance, any of which can fail in LPR.
- [Wu et al., Scientific Reports, 2021] — Found that weaker upper esophageal sphincter bolus transit on high-resolution impedance manometry correlated with higher (more severe) laryngopharyngeal reflux symptom scores.
David Gray
Content Researcher & Author
David Gray founded Wipeout Reflux to address a critical gap in reflux management. His research synthesizes over 100 peer-reviewed studies on laryngopharyngeal reflux (LPR), pepsin biology, and GERD pathophysiology. For LPR specifically—a condition most physicians misdiagnose—his work focuses on pepsin reactivation and why standard PPI therapy fails most patients. He develops evidence-based protocols targeting root causes of both LPR and GERD, integrating emerging research on sphincter dysfunction, dietary interventions, and newer clinical approaches. Wipeout Reflux represents practical application of clinical science for patients seeking real solutions.