
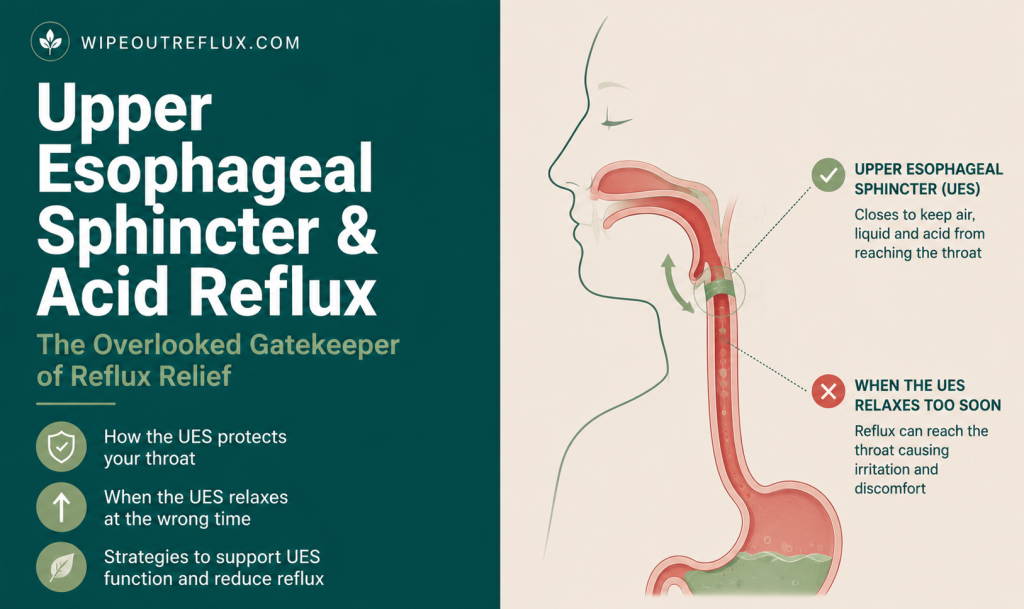
Most discussions of acid reflux focus on one valve — the lower oesophageal sphincter (LES), which separates the stomach from the oesophagus. When the LES relaxes inappropriately, stomach contents escape upward and you get GERD. It’s a well-established story. What’s far less discussed is the second valve: the upper oesophageal sphincter (UES), which sits at the top of the oesophagus, separating it from the throat and airway.
The UES is the anatomical difference between GERD and silent reflux (LPR). When the LES fails, you get acid in your oesophagus. When the UES also fails — or when its protective reflex underperforms — that acid and pepsin reach the throat, larynx, and airway. This is the mechanism behind every symptom cluster that makes LPR so confusing: no heartburn, but hoarseness, chronic cough, throat clearing, globus sensation, and post-nasal drip. The oesophagus may be largely unscathed; the throat takes the damage.
This article explains the UES in full — its anatomy, its protective reflex, what happens when it fails, and what that means practically for anyone managing silent reflux.
Key Takeaways
- The upper oesophageal sphincter (UES) is the second line of defence against reflux — it guards the throat from what the LES failed to contain
- The UES has a specific protective reflex (the esophago-UES contractile reflex, EUCR) that tightens the sphincter when refluxate is detected in the oesophagus below
- When this reflex underperforms in people with supraesophageal (LPR-type) reflux, the UES relaxes rather than contracts in response to acid exposure — allowing refluxate to breach the throat
- A high-resolution manometry study found abnormal UES function in approximately one-third of patients with LPR or GERD
- Throat tissue lacks the protective mechanisms the oesophagus has — no bicarbonate secretion, no acid-clearing peristalsis, no protective mucus layer — meaning even tiny reflux events cause disproportionate damage
- The UES can also become hypercontracted (spasm), which produces the globus sensation — a lump-in-throat feeling that often has nothing to do with a physical obstruction
- Standard 24-hour pH tests often miss UES-level events — which is why many LPR patients are told their tests are “normal”
- Reducing the reflux events that reach the UES — through diet, sleep positioning, and alginate barriers — is more reliably effective than trying to directly strengthen the UES
What Is the Upper Esophageal Sphincter?
The upper oesophageal sphincter is a ring of muscle located at the junction between the pharynx (throat) and the oesophagus, sitting roughly at the level of the C5–C6 vertebrae in the neck. Its primary component is the cricopharyngeus muscle, with contributions from the inferior pharyngeal constrictors and the upper fibres of the cervical oesophagus.
In its resting state, the UES maintains a constant contracted pressure — typically between 40 and 100 mmHg — that keeps the passage between the oesophagus and the throat closed. This resting tone is essential: it’s what prevents the contents of the oesophagus (and anything that has already refluxed up from the stomach) from entering the throat and airway. The UES relaxes rhythmically and transiently to allow swallowing, belching, and vomiting — and then immediately reseals.
Unlike the lower oesophageal sphincter, which is composed of smooth muscle and controlled by the autonomic nervous system, the UES is primarily composed of striated muscle and is under both voluntary and involuntary control. This dual control system is what makes it responsive to protective reflexes while also potentially trainable through exercises — though the evidence for exercise-based UES strengthening in reflux contexts is still limited.
Upper Esophageal Sphincter vs Lower Esophageal Sphincter: Two Different Valves, Two Different Problems
Understanding why LPR and GERD are clinically distinct requires understanding the roles of both sphincters as a two-valve system.
The lower oesophageal sphincter (LES) is the first guard. It sits at the bottom of the oesophagus, separating the stomach from the oesophageal column. When the LES relaxes inappropriately — through transient relaxations, reduced resting pressure, or structural issues like hiatal hernia — stomach contents escape upward into the oesophagus. This is GERD. The oesophagus has robust protective mechanisms: it secretes bicarbonate to neutralise acid, clears acid through peristaltic waves, and has a multilayer mucous lining. People with GERD can have significant acid exposure in the oesophagus and still experience only heartburn — because the oesophagus is built to resist it, up to a point.
The upper oesophageal sphincter is the second guard. Once refluxate is in the oesophagus, the UES is the last anatomical barrier preventing it from reaching the throat and larynx. If the UES is functioning well and its protective reflexes are intact, most oesophageal reflux events don’t result in pharyngeal exposure. If the UES fails — or if its reflex misfires — refluxate breaches the throat. This is LPR. And at the throat level, the tissue has almost none of the protective capacity the oesophagus has, which is why even tiny exposures cause significant damage.
Understanding this distinction is why the difference between GERD and LPR goes so much deeper than “one has heartburn and one doesn’t.” They are different anatomical failures with different symptom clusters, different tissue damage profiles, and different treatment responses.
The UES Protective Reflex: The Defence Most Pages Miss
The UES does more than passively sit closed. It has a specific, active protective mechanism designed to respond to reflux events below it — and understanding this reflex is the key to understanding why LPR is a distinct pathological state.
When refluxate (acid, pepsin, and gastric contents) moves upward in the oesophagus and distends the oesophageal wall, it stimulates mechanoreceptors in the oesophageal muscle. These receptors trigger a reflexive contraction of the UES — a tightening response that specifically counteracts the upward pressure of the approaching refluxate. This is the esophago-UES contractile reflex (EUCR), and it is mediated through the vagus nerve [Lippincott M. and Velanovich V., Annals of Esophagus, 2022].
In healthy individuals, this reflex is the reason that the vast majority of reflux events — including quite significant ones — don’t result in LPR symptoms. The oesophagus detects the ascending refluxate, signals the UES to contract harder, and the refluxate is confined below the throat. The EUCR is, in effect, the body’s dedicated last-resort mechanism against the very event that causes LPR.
There is a paired reflex, the esophago-UES relaxation reflex (EURR), which does the opposite — it allows the UES to briefly relax to permit gas venting (belching). When the balance between these two reflexes is disrupted, the UES opens at the wrong times: relaxing in response to refluxate rather than contracting. Research has shown that patients with supraesophageal reflux disease — the clinical umbrella for LPR — have demonstrably impaired UES contractile reflexes compared to healthy controls and even compared to typical GERD patients [Gastroenterology, 2015]. The protective mechanism is specifically, measurably deficient in these patients.
Upper Esophageal Sphincter Dysfunction and Silent Reflux (LPR)
LPR occurs precisely at the intersection of LES dysfunction and UES protective reflex failure. Refluxate escapes the stomach (LES problem), enters the oesophagus, approaches the UES — and rather than triggering a defensive tightening, the UES either fails to contract strongly enough or, in some cases, actually relaxes. The refluxate passes through into the pharynx, larynx, and sometimes the lower airway.
What makes this particularly important for people who’ve been dismissed by doctors is the measurability of this dysfunction. High-resolution esophageal manometry (HREM) can directly measure UES pressure, resting tone, and reflex responses. A retrospective study of 220 patients evaluated for GERD or LPR symptoms — using HREM, ambulatory pH monitoring, and endoscopy — found that abnormal UES function was present in approximately one-third of the overall group [Benjamin T. et al., Scandinavian Journal of Gastroenterology, 2017]. This is a meaningful proportion. It means that a substantial percentage of people with LPR and GERD have a measurable, documented abnormality in UES function — and that this is not simply a subjective experience or a “functional” complaint without a physical basis.
The consequence of UES breach is the full LPR symptom cluster: hoarseness, throat clearing, chronic cough, post-nasal drip sensation, globus, and in more severe cases, recurrent throat infections or airway irritation. All of these are downstream effects of a single anatomical event — refluxate passing through a valve that should have held it back.
Why Even Tiny Reflux Damages the Throat
One of the most clinically important — and most frequently overlooked — aspects of LPR is why the symptoms can be so severe when the reflux events themselves seem relatively minor. Someone with GERD might have a pH probe recording significant acid exposure in the oesophagus and experience manageable heartburn. Someone with LPR might have what appears to be minimal reflux reaching the throat and still have persistent hoarseness and throat inflammation that takes months to resolve.
The explanation lies in the difference between oesophageal and laryngopharyngeal tissue. The oesophagus has evolved alongside reflux and has multiple layers of defence: a multilayer stratified epithelium, bicarbonate secretion from submucosal glands, continuous peristaltic clearing of acid, and salivary bicarbonate delivered with every swallow. These mechanisms allow the oesophagus to tolerate significant acid exposure without immediately sustaining damage.
The throat — larynx, pharynx, vocal folds — has none of these mechanisms in any meaningful concentration. Laryngeal epithelium is thin, lacks the same mucous protection, has minimal local buffering capacity, and no clearance mechanism. When refluxate reaches this tissue, there is nothing to neutralise it, wash it away, or buffer the pH. The exposure lingers. Pepsin — the enzyme carried with acid refluxate from the stomach — embeds in the epithelial cells and persists, reactivating every time the local pH drops below about 4. A single significant reflux event reaching the larynx can cause more tissue irritation than dozens of oesophageal events that are adequately cleared. My detailed guide to neutralising pepsin in the throat explains this mechanism and why treatment approaches need to account for it.
This is the most useful explanation of why “silent reflux” is silent: the oesophagus may not be generating heartburn because its defences are handling the acid reasonably well. But the throat tissue is entirely undefended, and even small volumes of refluxate passing through an underperforming UES cause real, cumulative inflammation.
Upper Esophageal Sphincter Spasm: When the UES Is Too Tight
Not all UES dysfunction presents as failure to close. The UES can also become hypercontracted — producing a state of elevated resting pressure and reduced relaxation — which creates a different set of symptoms.
UES spasm or hypertension is one of the primary mechanisms behind globus pharyngeus — the persistent sensation of a lump, tightness, or something stuck in the throat that doesn’t go away with swallowing. When the UES detects refluxate below it (or anticipates it, based on learned sensitisation), it may contract excessively as a protective overresponse. The cricopharyngeus muscle enters a state of persistent elevated tone. Swallowing feels difficult or requires effort. The throat feels tight or constricted. Food sometimes feels like it catches.
The important clinical point about globus is that it can coexist with, or even be caused by, LPR — not as a structural obstruction but as a functional one driven by UES hypercontraction. My guide to the lump-in-throat sensation from reflux covers the full picture of globus in the reflux context. Treating the underlying LPR — reducing the frequency and volume of refluxate reaching the UES — often resolves the globus sensation, because the hypercontraction reflex no longer has a reason to fire.
How to Support Upper Esophageal Sphincter Function
The most honest framing here is that the most effective way to protect the UES is to reduce the frequency and volume of reflux events that challenge it — rather than trying to directly strengthen the sphincter in isolation. The UES doesn’t fail in a vacuum; it fails under sustained stimulus from repeated reflux events. Reduce those events, and the UES has less to contend with.
Dietary and Lifestyle Reduction of Reflux Load
The primary lever. Reducing the frequency of LES relaxations and the volume of gastric contents available to reflux directly reduces the frequency of UES challenges. The Wipeout Diet Plan provides the most comprehensive framework for this — covering dietary triggers, meal timing, portion size, and the eating patterns that generate the most gastric pressure. For specific food and drink safety ratings with pH values, the Wipeout Reflux Food Reference Guide is the practical daily reference.
Sleep Positioning
Nocturnal reflux is particularly damaging for the UES because lying flat removes the gravitational barrier that helps keep refluxate below the throat. Head elevation of 15–20cm and left-side sleeping both meaningfully reduce pharyngeal acid exposure during sleep. See my guide to the best sleeping position for silent reflux for evidence-based detail on positioning strategy.
Alginate-Based Treatments
Alginates like Gaviscon Advance form a floating raft on the surface of stomach contents that physically blocks refluxate from escaping through the LES — and therefore reduces the volume and frequency of refluxate that the UES then needs to contend with. For LPR specifically, alginates address the pepsin component as well as the acid component, making them more targeted than PPIs for throat-level symptoms. My Gaviscon Advance guide covers dosing and timing for LPR contexts.
Pharyngeal Exercise Devices
The IQoro is a neuromuscular training device that applies resistance to the oropharyngeal muscles, including those involved in UES function. It was primarily developed for dysphagia and swallowing disorders, and the evidence base in reflux contexts is still developing — but it represents one of the few interventions with a specific UES-strengthening mechanism. My IQoro review covers the current evidence in detail.
Avoid UES-Relaxing Substances
Caffeine and alcohol both reduce muscle tone in the GI tract, including the UES and LES. For LPR specifically — where the UES is already compromised — reducing caffeine intake and eliminating alcohol represents a meaningful mechanical intervention that goes beyond just “avoiding triggers.”
UES and LPR Diagnosis: Why Tests Often Miss It
One of the most common — and most frustrating — experiences for people with LPR is being told their reflux tests came back normal. Understanding why this happens requires understanding what standard reflux testing actually measures.
The conventional 24-hour pH monitoring test uses a probe placed in the distal oesophagus — approximately 5 centimetres above the LES. It measures acid exposure at that location. It doesn’t monitor pharyngeal pH. It doesn’t measure UES function. It can completely miss LPR events, particularly if the refluxate is weakly acidic or non-acidic (containing pepsin but not at pH <4), or if the reflux events are intermittent and don’t accumulate enough exposure time over the 24-hour period to cross the threshold for an abnormal result.
More advanced investigations that can actually capture UES-level events include:
- High-resolution esophageal manometry (HREM): Directly measures UES resting pressure, relaxation, and reflex responses. The study by Benjamin et al. (2017) used HREM specifically to document the one-third prevalence of UES abnormality — a finding that a standard pH study would not have captured
- Dual-sensor pH monitoring: Places probes both distally (standard position) and proximally in the pharynx. Catches pharyngeal acid exposure that a distal probe alone misses
- Multichannel intraluminal impedance with pH (MII-pH): Detects both acidic and non-acidic reflux events, and can track the upward movement of refluxate in real time — including whether it reaches the UES or above
- Pepsin testing (Peptest): A saliva or throat swab test that detects the presence of pepsin — which should not be present in throat secretions unless LPR has occurred. My article on the Peptest covers this in full
If you’ve been told your reflux tests are normal but continue to have throat symptoms consistent with LPR, the investigation may simply not have been designed to detect the problem you have. That’s not a dismissal of your experience — it’s a gap in the standard diagnostic pathway.
Frequently Asked Questions
What is the upper esophageal sphincter?
The upper oesophageal sphincter is a ring of muscle at the junction between the throat and the oesophagus, primarily composed of the cricopharyngeus muscle. It stays contracted in its resting state to prevent oesophageal contents from reaching the throat and airway, and relaxes briefly during swallowing, belching, and vomiting.
How does the UES differ from the LES?
The LES (lower oesophageal sphincter) sits at the stomach-oesophagus junction and prevents stomach contents from escaping upward into the oesophagus — its failure causes GERD. The UES sits at the oesophagus-throat junction and prevents oesophageal contents from reaching the throat — its failure causes LPR/silent reflux. They are different muscles at different anatomical levels, with different tissue compositions and different control mechanisms.
What causes upper esophageal sphincter dysfunction?
The most relevant mechanism for LPR is impairment of the UES’s protective contractile reflex (EUCR) — the normal tightening response to ascending refluxate. When this reflex underperforms, refluxate breaches the sphincter and reaches the throat. Chronic acid exposure can sensitise the oesophageal receptors involved, progressively impairing the reflex over time. Other causes of UES dysfunction include neurological conditions, ageing, and certain medications.
Can you strengthen the upper esophageal sphincter?
Directly strengthening the UES through targeted exercises is an emerging area with limited robust evidence in reflux contexts. Pharyngeal resistance training devices like IQoro work on the oropharyngeal muscle system and may support UES function. The most effective current approach is reducing the reflux events that challenge the UES — through diet, positioning, and barrier treatments — so the sphincter has less to contend with while any recovery occurs.
What does UES spasm feel like?
UES spasm or hypertension typically presents as a persistent lump, tightening, or pressure sensation in the throat — the globus sensation. It may worsen with reflux episodes and feel unrelated to meals. Swallowing may feel effortful or incomplete. It can also present as intermittent throat constriction or difficulty initiating a swallow. These symptoms often resolve when the underlying LPR driving the hypercontraction reflex is properly managed.
Why do standard reflux tests miss LPR?
Standard 24-hour pH tests measure acid exposure in the distal oesophagus — not at the UES or in the pharynx. LPR events that don’t generate enough oesophageal acid exposure to cross the abnormal threshold will be missed entirely. Dual-sensor pharyngeal pH monitoring, MII-pH testing that detects non-acidic reflux, or HREM for direct UES pressure measurement are more appropriate investigations when LPR is suspected but standard tests are normal.
Is the globus sensation from the throat always caused by reflux?
Not always — but LPR is one of the most common causes and is frequently missed. The globus sensation can also be caused by anxiety, post-nasal drip, thyroid disorders, and occasionally structural oesophageal issues. When throat symptoms persist without obvious cause, investigating for LPR through more sensitive testing (pharyngeal pH, impedance, or pepsin testing) is a productive next step. My full guide to the lump-in-throat sensation from reflux covers the diagnostic approach in detail.
Conclusion
The upper oesophageal sphincter is the missing piece in most people’s understanding of their own reflux. GERD is a familiar concept — acid from the stomach, heartburn, PPIs. LPR is far less understood, partly because it requires understanding not one valve but two: what the LES failed to contain, and what the UES failed to keep out of the throat.
The vagal protective reflex that the UES deploys when refluxate approaches is a remarkable piece of physiology — and when it underperforms, the downstream consequences are the entirety of the silent reflux symptom picture. The one-third prevalence of measurable UES abnormality in LPR and GERD patients is not a small finding. It gives a tangible, testable mechanism to symptoms that have too often been dismissed as functional or psychosomatic.
Understanding this anatomy is the foundation for understanding everything else on this site. The complete guide to LPR builds directly on this mechanism — explaining how pepsin reaches and damages the throat once the UES is breached, and what the full treatment picture looks like. And for the foundational dietary framework that reduces the reflux events challenging the UES in the first place, the Wipeout Diet Plan covers the evidence-based approach to dietary management of both GERD and LPR.
Research & References
Benjamin T., Zackria S., Lopez R., Richter J., Thota P.N. (2017). Upper esophageal sphincter abnormalities and high-resolution esophageal manometry findings in patients with laryngopharyngeal reflux. A retrospective study of 220 patients evaluated with HREM, ambulatory pH monitoring, and endoscopy found that abnormal UES function was present in approximately one-third of patients with LPR or GERD across all three symptom groups studied. [Benjamin T. et al., Scandinavian Journal of Gastroenterology, 2017]
Lippincott M. and Velanovich V. (2022). The upper esophageal sphincter in gastroesophageal reflux disease. This review describes the vagally mediated esophago-UES contractile reflex (EUCR) as the primary protective mechanism preventing oropharyngeal reflux, and the esophago-UES relaxation reflex (EURR) as its paired reflex allowing gas venting. The UES responds to liquid refluxate with a contractile response in healthy, supine subjects — a mechanism distinct from belch relaxation. [Lippincott M. and Velanovich V., Annals of Esophagus, 2022]
Impaired upper esophageal sphincter reflexes in patients with supraesophageal reflux disease. Gastroenterology, 2015. (PMID: 26188682) This study found that significantly fewer patients with supraesophageal reflux disease (SERD/LPR) exhibited UES contractile reflexes in response to simulated acid reflux events, compared to healthy controls or standard GERD patients. Only patients with SERD had abnormal UES relaxation responses to rapid distension — a pattern that could predispose them to esophagopharyngeal reflux. [Gastroenterology, 2015]
David Gray
Content Researcher & Author
David Gray founded Wipeout Reflux to address a critical gap in reflux management. His research synthesizes over 100 peer-reviewed studies on laryngopharyngeal reflux (LPR), pepsin biology, and GERD pathophysiology. For LPR specifically—a condition most physicians misdiagnose—his work focuses on pepsin reactivation and why standard PPI therapy fails most patients. He develops evidence-based protocols targeting root causes of both LPR and GERD, integrating emerging research on sphincter dysfunction, dietary interventions, and newer clinical approaches. Wipeout Reflux represents practical application of clinical science for patients seeking real solutions.