
GERD and LPR are both forms of acid reflux — but they are not the same condition, they cause different symptoms, they affect different parts of the body, and crucially they require different treatment approaches. Confusing the two is one of the most common reasons people end up on treatment plans that don’t work for them.
If you have been diagnosed with one and the treatment isn’t helping, or if you are trying to figure out which one you actually have, this article will give you a clear picture of both conditions, how to tell them apart, and what to do about each.
Key Takeaways:
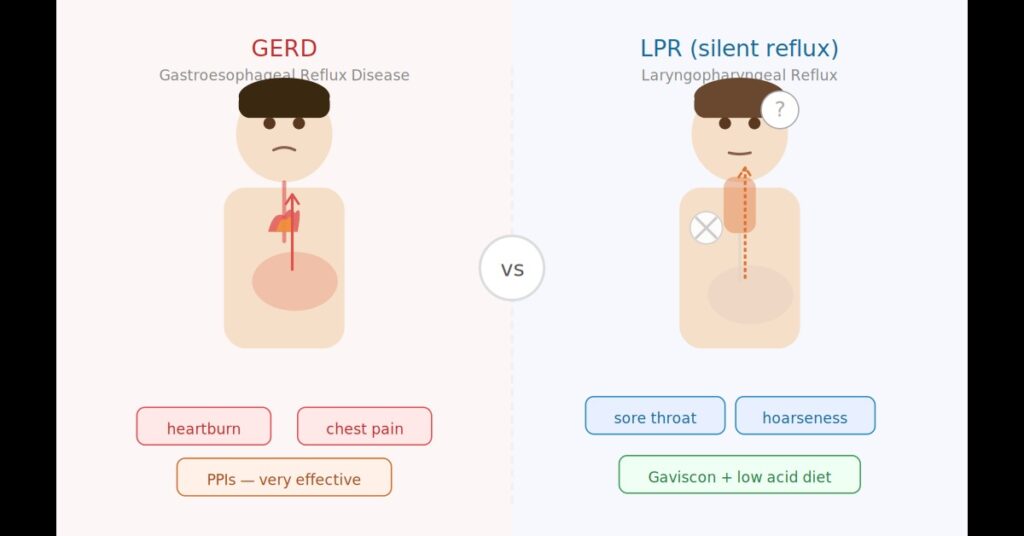
- GERD symptoms appear mainly in the chest — heartburn, indigestion, chest pain
- LPR symptoms appear mainly in the throat — sore throat, hoarseness, cough, mucus
- Most people with LPR have no heartburn at all — that’s why it’s called silent reflux
- PPIs work well for GERD but have been proven in clinical trials to be no better than placebo for LPR
- LPR is primarily driven by pepsin, not just acid — which changes everything about how it needs to be treated
- You can have both conditions at the same time
What is GERD?
GERD (Gastroesophageal Reflux Disease) is the most common form of acid reflux. It occurs when the lower esophageal sphincter (LES) — the valve between the stomach and the oesophagus — fails to close properly and allows stomach acid to reflux back up into the oesophagus.
The oesophagus is the tube that connects your throat to your stomach. In GERD, the acid stays mostly within the oesophagus rather than travelling further upward. Because the oesophageal lining comes into direct contact with stomach acid, it causes irritation and inflammation — and you feel this as heartburn, that burning sensation in the middle of the chest.
GERD is extremely common. Population-based research suggests that around 19-28% of adults in North America experience typical GERD symptoms at least weekly, making it the most frequently diagnosed gastrointestinal condition in the western world.
GERD Symptoms
- Heartburn — the classic burning sensation in the chest, usually after eating or when lying down
- Regurgitation — acid or food coming back up into the mouth
- Chest pain — sometimes severe enough to be mistaken for a cardiac problem
- Difficulty swallowing — caused by oesophageal inflammation or narrowing
- Nausea — particularly after meals
- Bloating and belching
- Worsening symptoms when lying down — particularly at night
GERD typically causes visible damage to the oesophagus over time. If left untreated, it can lead to oesophagitis (inflammation of the oesophagus), oesophageal strictures, and in serious cases Barrett’s oesophagus — a precancerous change to the oesophageal lining.
What is LPR?
LPR (Laryngopharyngeal Reflux), also known as silent reflux, is a different form of acid reflux where the stomach contents travel further — past the oesophagus, through the upper oesophageal sphincter (UES), and all the way up into the throat, larynx (voice box), sinuses and sometimes the ears.
The key difference is where the reflux ends up. In GERD it stays in the oesophagus. In LPR it reaches the throat and above. And because the throat and larynx have almost no natural protection against stomach acid and pepsin, even very small amounts of reflux reaching these areas can cause significant inflammation and a wide range of symptoms — most of which have nothing to do with the chest.
A landmark paper by Koufman et al. established that LPR and GERD are genuinely different conditions with different patterns, mechanisms and treatment requirements, and that the standard gastroenterology model of reflux disease does not apply to LPR. This distinction is now supported by the 2024 IFOS international consensus which formally defines LPR as a separate clinical entity.
LPR Symptoms
- Persistent sore or irritated throat — the most common symptom
- Constant need to clear the throat
- Hoarseness or voice changes
- Chronic cough — usually dry, worse after eating
- Lump in the throat feeling (globus sensation)
- Excess mucus in the throat
- Post nasal drip
- Sinus congestion
- Ear pain or discomfort
- Difficulty breathing — particularly when inhaling
- Dental erosion
For a detailed breakdown of each symptom and what causes it, check my article on LPR symptoms.
The Most Important Difference — LPR Usually Has No Heartburn
This is the single most important distinction to understand and the main reason LPR gets missed so often. The majority of people with LPR do not experience heartburn. This is what earns it the name silent reflux — the reflux is happening but the chest symptoms that would normally alert someone to seek help are absent.
According to StatPearls (2025), many patients with LPR report no heartburn, regurgitation, chest pain, nausea or vomiting — supporting the idea that GERD and LPR are genuinely separate conditions. And a 2024 review in the World Journal of Gastroenterology confirms that LPR occurs predominantly in the upright position during the day, whereas GERD tends to be worse at night when lying down — another key differentiator.
This absence of heartburn is exactly why so many people with LPR spend months or years going from doctor to doctor without the right diagnosis. If you have persistent throat and voice symptoms but no chest symptoms, LPR is the more likely explanation — not allergies, not a persistent cold, and not just stress.
Why the Throat is So Vulnerable in LPR
You might wonder — if both conditions involve reflux, why does LPR cause so much damage when it seems like such a small amount of material is reaching the throat?
The answer is that the oesophagus has several built-in defences against acid. It clears acid quickly through peristalsis, it produces bicarbonate-containing saliva to neutralise acid, and the oesophageal lining itself has some resistance to acid exposure. The throat and larynx have almost none of these defences. The laryngeal mucosa is exquisitely sensitive — even a tiny amount of pepsin or acid making contact with it can trigger a significant inflammatory response.
As Koufman’s research established, the laryngopharyngeal epithelium is far more susceptible to reflux-related tissue injury than the oesophageal epithelium. This is why LPR can cause significant symptoms even when the reflux events are infrequent or the acid is only mildly acidic.
The Role of Pepsin — Why LPR is Different at a Cellular Level
Beyond where the reflux ends up, there is another crucial difference between GERD and LPR — and that is the role of pepsin.
In GERD, acid is the primary cause of damage. Reducing acid with PPIs significantly reduces oesophageal damage and symptom relief for most GERD patients. This is why PPIs work well for GERD.
In LPR, pepsin — a digestive enzyme that travels up with the acid — is the primary driver of damage. Pepsin causes direct tissue inflammation in the throat even in conditions that are only mildly acidic, and it can remain dormant in throat cells for 24 to 48 hours after a reflux episode. If you eat or drink anything acidic during that time, the pepsin gets reactivated and symptoms flare — even without any further reflux occurring.
This is why simply reducing stomach acid with PPIs does not solve LPR. The pepsin is still there, still getting reactivated, and still causing damage. A 2024 study published in Cytokine (Tan et al.) confirmed that pepsin triggers an inflammatory cascade in the larynx even in only mildly acidic conditions, explaining exactly why acid suppression alone is insufficient for LPR.
GERD vs LPR — A Clear Comparison
| GERD | LPR (Silent Reflux) | |
|---|---|---|
| Where reflux reaches | Oesophagus | Throat, larynx, sinuses, ears |
| Main symptom | Heartburn | Sore throat, hoarseness, throat clearing |
| Heartburn present? | Usually yes | Usually no — that’s why it’s “silent” |
| When worst | Night, lying down | Daytime, upright |
| Primary damaging agent | Acid | Pepsin (digestive enzyme) |
| Oesophagitis common? | Yes | Usually no |
| Do PPIs help? | Yes — very effectively | No — proven no better than placebo |
| Best medication | PPIs, H2 blockers | Gaviscon Advance (UK version) |
| Diet approach | Avoid trigger foods | Avoid foods with pH below 5 (pepsin reactivation) |
Can You Have Both GERD and LPR at the Same Time?
Yes — and it’s fairly common. Some people have reflux that causes symptoms both in the oesophagus (heartburn, chest pain) and in the throat (hoarseness, throat clearing). In these cases both conditions need to be addressed.
A study published in the Indian Journal of Otolaryngology (2019) found that of 100 patients presenting with reflux symptoms, 40 had both GERD and LPR simultaneously — the largest group in the study. If you have both, treatment generally needs to address both — PPIs may help the GERD component while Gaviscon Advance and diet changes target the LPR component.
Why the Treatment Difference Matters So Much
The treatment difference between GERD and LPR is where the confusion causes the most real-world harm. Most doctors — including many gastroenterologists and ENT specialists — treat both conditions with PPIs. For GERD this is appropriate and effective. For LPR it is not, and the evidence is unambiguous on this.
The landmark TOPPITS trial published in the BMJ (O’Hara et al., 2021) — the largest clinical trial of its kind with 346 patients — found that PPIs were no better than placebo for treating persistent throat symptoms related to LPR. The 2024 IFOS international consensus now formally states that acid suppression should not be the first-line treatment for patients with isolated LPR symptoms. And a 2025 systematic review by Lechien et al. confirmed that more than 50% of otolaryngologists still treat LPR exclusively with PPIs — demonstrating how far behind clinical practice still lags behind the evidence.
If you have been given PPIs for what seems like throat symptoms and they are not helping, this is not a failure of treatment — it is likely the wrong treatment for your condition.
How Each Condition is Best Treated
GERD Treatment
For GERD, PPIs are the gold standard medical treatment and do work well for most people. Diet changes are also important — particularly avoiding the classic trigger foods like caffeine, alcohol, fatty foods, chocolate and spicy food, and not eating close to bedtime. Losing weight if overweight can also significantly help GERD.
For more detail check my article on acid reflux and GERD.
LPR Treatment
LPR needs a completely different approach. The two most effective treatments are:
1. Gaviscon Advance (UK version) — this creates a physical alginate raft that prevents reflux from reaching the throat and filters pepsin. It has solid clinical trial evidence behind it. Taken 15-30 minutes after meals and before bed. Make sure you use the UK version — the US version has different ingredients and is far less effective for LPR. For more detail check my article on Gaviscon Advance for LPR.
2. A low acid diet — specifically avoiding foods and drinks with a pH below 5. This is about preventing pepsin reactivation, not just reducing acid. A clinical study by Koufman found 95% of LPR patients improved on a strict low acid diet, including those who had failed PPI treatment. For full guidance check my LPR diet article.
Alkaline water with a pH of 8 or above is also worth adding — it has been shown to directly deactivate pepsin in the throat. Check my article on alkaline water for LPR.
For a complete guide to treating LPR check my article on silent reflux treatment.
How to Know Which One You Have
The symptom pattern is usually the clearest guide:
- If your main symptoms are heartburn and chest pain — GERD is more likely
- If your main symptoms are throat, voice and sinus related with no heartburn — LPR is more likely
- If you have both chest and throat symptoms — you may have both
The RSI (Reflux Symptom Index) test is the most reliable self-assessment tool for LPR. It scores 9 key LPR symptoms and a score above 13 is considered strongly suggestive of LPR. I have built it directly into my site — take the RSI test here.
For a more formal diagnosis, GERD is typically confirmed through endoscopy or oesophageal pH monitoring. LPR diagnosis involves laryngoscopy to look for signs of inflammation in the throat and larynx, sometimes combined with a 24-hour pH impedance study. A Peptest — a saliva test that detects pepsin — can also support an LPR diagnosis. For more information on the best diagnostic test for LPR check my article on Restech pH monitoring.
Frequently Asked Questions
Is LPR the same as GERD?
No. While both involve acid reflux, they are distinct conditions that affect different parts of the body, cause different symptoms and require different treatment. GERD causes chest symptoms like heartburn. LPR causes throat symptoms like hoarseness, sore throat and chronic cough. Most people with LPR have no heartburn at all.
Can you have LPR without GERD?
Yes, absolutely. Many people with LPR have no oesophageal symptoms and no GERD diagnosis. The reflux in LPR may bypass the oesophagus and reach the throat without causing the typical GERD symptoms. Research supports that LPR and GERD are genuinely separate conditions that can occur independently.
Why do PPIs help GERD but not LPR?
GERD is primarily driven by acid, so reducing acid with PPIs directly addresses the cause. LPR is primarily driven by pepsin — a digestive enzyme that causes damage even in weakly acidic conditions. PPIs reduce acid but don’t stop pepsin from causing damage, which is why they consistently fail in clinical trials for LPR.
What is the difference between silent reflux and acid reflux?
Silent reflux is another name for LPR. It’s called silent because the heartburn that typically signals acid reflux is absent. The reflux is still happening — it’s just not causing chest symptoms because it’s reaching the throat rather than staying in the oesophagus. Regular acid reflux or GERD typically does cause heartburn.
Can GERD turn into LPR?
It’s possible for someone with GERD to also develop LPR if reflux begins to travel higher and reach the throat, particularly if the upper oesophageal sphincter becomes compromised. However LPR can also develop independently without any prior GERD diagnosis.
How do I know if I have GERD or LPR?
Look at where your symptoms are. Heartburn and chest discomfort point to GERD. Persistent sore throat, hoarseness, throat clearing, chronic cough and sinus problems without heartburn point to LPR. Take the RSI test here for a quick and reliable self-assessment for LPR, or check my article on LPR symptoms for a full breakdown.
Conclusion
GERD and LPR are related but genuinely different conditions. GERD causes heartburn and oesophageal symptoms and responds well to PPIs. LPR causes throat and voice symptoms, rarely causes heartburn, is driven primarily by pepsin rather than acid, and does not respond to PPIs — it needs a completely different treatment approach.
Getting this distinction right is the difference between years of failed treatment and actually getting better. If you have throat symptoms and have been given PPIs without success, there is a good chance you have LPR rather than — or as well as — GERD, and the treatment needs to change.
For next steps take the RSI test, read my complete LPR guide and my article on silent reflux treatment. And if you want a tailored treatment plan based on your specific situation consider a private consultation.
Related articles:
- The Complete Guide to LPR — Causes, Symptoms and Treatment
- Acid Reflux and GERD — The Complete Guide
- LPR Symptoms — The Complete Guide
- Silent Reflux Treatment — What Actually Works
- LPR Diet — What to Eat, What to Avoid and What to Drink
- RSI Test — Do You Have LPR?
- Why Gaviscon Advance is the Best Option for LPR
- Getting Off PPIs Safely — Acid Rebound Guide
References
- Koufman JA et al. (2002) “Laryngopharyngeal reflux is different from classic gastroesophageal reflux disease.” Ear, Nose and Throat Journal. PubMed
- Lechien JR et al. (2024) “The Dubai definition and diagnostic criteria of laryngopharyngeal reflux: the IFOS consensus.” The Laryngoscope, 134(4):1614-1624. PubMed
- Tan JJ et al. (2024) “Pepsin-mediated inflammation in laryngopharyngeal reflux via the ROS/NLRP3/IL-1β signaling pathway.” Cytokine, 178:156568. PubMed
- O’Hara J et al. (2021) “Use of proton pump inhibitors to treat persistent throat symptoms: multicentre, double blind, randomised, placebo-controlled trial.” BMJ, 372:m4903. BMJ
- Lechien JR et al. (2025) “Treatment for Laryngopharyngeal Reflux Disease: A Systematic Review of Controlled Studies.” Journal of Otolaryngology — Head and Neck Surgery. Full text
- Koufman JA. (2011) “Low-acid diet for recalcitrant laryngopharyngeal reflux.” Annals of Otology, Rhinology and Laryngology, 120(5):281-287. PubMed
- Brown J, Shermetaro C. (2025) “Laryngopharyngeal Reflux.” StatPearls. NCBI Bookshelf
- Sanu A, Eccles R. (2018) “Focus on gastroesophageal reflux (GER) and laryngopharyngeal reflux (LPR): new pragmatic insights in clinical practice.” Journal of Biological Regulators and Homeostatic Agents. PubMed
- Chandrasekhar SS et al. (2019) “Laryngopharyngeal Reflux and GERD: Correlation Between RSI and RFS.” Indian Journal of Otolaryngology. PMC
David Gray
Content Researcher & Author
David Gray founded Wipeout Reflux to address a critical gap in reflux management. His research synthesizes over 100 peer-reviewed studies on laryngopharyngeal reflux (LPR), pepsin biology, and GERD pathophysiology. For LPR specifically—a condition most physicians misdiagnose—his work focuses on pepsin reactivation and why standard PPI therapy fails most patients. He develops evidence-based protocols targeting root causes of both LPR and GERD, integrating emerging research on sphincter dysfunction, dietary interventions, and newer clinical approaches. Wipeout Reflux represents practical application of clinical science for patients seeking real solutions.
Thanks very much for all the valuable information on your site. I have found it very helpful. About the distinction between LPR and GERD: I have a hard time understanding how acid reflux can bypass the esophagus on the way to the throat. If acid is passing through the esophagus, wouldn’t it necessarily cause esophagitis? Many thanks for helping me with this question.
Thanks so much — really glad the site’s been helpful.
Great question. You’re right that the acid doesn’t skip the esophagus — it travels up through it. The difference is that your esophagus is built to handle brief acid contact and your throat isn’t.
Your esophagus has a tough lining, plus a natural squeezing motion that sweeps acid back down in seconds and saliva that neutralises the rest. So a quick splash usually passes through without causing damage. Your throat has none of that protection and much more delicate tissue, so the same splash irritates it easily.
Two more things: LPR reflux is often a brief mist rather than the pooling reflux you get lying down with GERD, so it barely lingers in the esophagus. And the real culprit is often pepsin, not just acid — it rides up, lands on your throat, and causes trouble there even when acid is low.
That’s why so many of us with LPR have a normal endoscopy and no heartburn — the damage is happening above the esophagus, not in it.
Hope that helps.
David
Is it possible that, taking Pantoprazole 40mg actually increases LPR symptoms especially coughing ?
Potentially. If you have low stomach acid for example, taking the PPI may make it worse. It can also make other issues worse like gut issues or motility which can worsen LPR for some people.
Pain when swallow saliva is sign of LPR?it comes and goes i am talking antibiotic for that with nexium
It could be but it’s hard to say for certain just on that one symptom.