
If you’ve tried to come off PPIs and felt dramatically worse — heartburn out of nowhere, acid refluxing constantly, symptoms that seem far worse than before you started the medication — that’s not your reflux getting worse. That’s acid rebound. And understanding what it actually is makes the whole experience much less frightening, and much more manageable.
I went through this myself. I stopped omeprazole abruptly after being on 40mg and ended up in A&E twice. I didn’t know what acid rebound was. Once I understood the mechanism and did it properly the second time — slowly, with the right support in place — it was a completely different experience.
This article covers exactly what acid rebound is, why it happens, how long it lasts, and the step-by-step method I recommend for coming off PPIs with the least disruption possible.
Key Takeaways:
- Acid rebound (rebound acid hypersecretion) is a well-documented physiological response to stopping PPIs — it is not your original condition getting worse
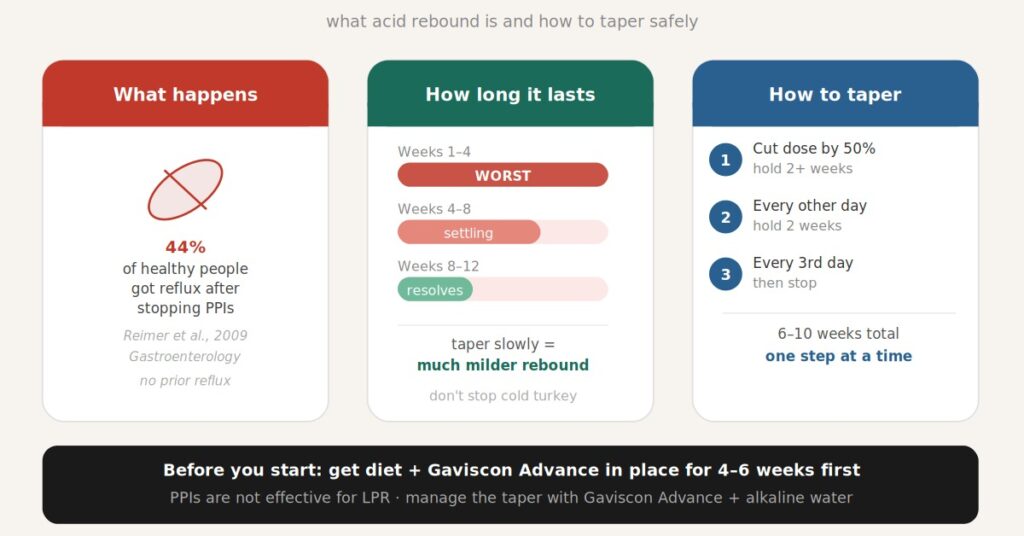
- 44% of healthy people with no prior reflux developed acid-related symptoms after stopping PPIs in a controlled trial — this effect is caused by the medication withdrawal, not by underlying disease
- Symptoms typically peak in weeks 1 to 4 after stopping and can last up to 8 to 12 weeks
- Tapering slowly over several weeks produces fewer symptoms than stopping abruptly — always taper rather than stopping cold turkey
- The best bridging agents during a taper are Gaviscon Advance (UK version) and H2 blockers like famotidine — used to manage symptoms while the stomach resets
- PPIs are largely ineffective for LPR — the evidence consistently shows they perform no better than placebo for throat symptoms
- Get the low acid diet in place for at least 4 to 6 weeks before starting your taper — this makes the process significantly easier
What Is Acid Rebound and Why Does It Happen?
Acid rebound — formally called rebound acid hypersecretion (RAHS) — happens because PPIs suppress stomach acid so effectively that the stomach adapts by upregulating its acid-producing capacity. When you stop the PPIs, that suppression is removed but the upregulated capacity remains — temporarily producing more acid than before you started.
Here’s the mechanism in plain terms. PPIs work by blocking proton pumps on the acid-producing cells in the stomach lining. When acid is persistently suppressed, the stomach responds by raising gastrin levels — a hormone that signals for more acid production. Elevated gastrin causes the acid-producing cells to multiply and become more active. So when the PPIs stop, you have a stomach that is now primed to produce significantly more acid than it was before you started the medication. That surge is rebound acid hypersecretion.
This is not your underlying condition getting worse. It is a temporary pharmacological withdrawal effect caused by the medication itself.
The most striking evidence for this comes from a 2009 controlled trial published in Gastroenterology by Reimer et al. Healthy volunteers with no history of reflux took esomeprazole 40mg daily for 8 weeks. After stopping, 44% developed acid-related symptoms including heartburn and regurgitation — compared to only 15% in the placebo group. These were people who had never had reflux in their lives. The medication caused the rebound, not any underlying disease.
A 2024 review published in the International Journal of Molecular Sciences (Namikawa & Björnsson) confirmed this mechanism is well-established and that rebound acid hypersecretion is one of the significant adverse effects of long-term PPI use that is still widely underappreciated by both patients and clinicians. PMID 38791497
PPIs and LPR: Why You Probably Shouldn’t Be on Them Long-Term
PPIs are not an effective treatment for LPR. This is one of the most important things I want people to understand — not just because of the rebound issue, but because staying on PPIs long-term for LPR means accepting side effects and dependency for a medication that isn’t doing what you think it’s doing.
The evidence is consistent: multiple studies have shown that PPIs perform no better than placebo for LPR symptoms. The reason is straightforward — LPR is primarily driven by pepsin reaching the throat, not by acid levels in the stomach. PPIs suppress acid but do nothing to stop pepsin from refluxing. The pepsin continues to reach the throat regardless, continues to cause inflammation, and the symptoms persist. For more on this see my silent reflux treatment guide.
So most people with LPR who are on PPIs are taking medication that isn’t treating their actual problem — and then going through a difficult rebound when they try to stop. The sooner you can come off them safely and shift to an approach that actually works for LPR, the better.
How Long Does Acid Rebound Last?
Acid rebound typically lasts between 4 and 12 weeks after stopping PPIs, depending on how long you were on them and at what dose. The symptoms are generally worst in the first 2 to 4 weeks and then gradually settle as the stomach’s acid-producing capacity returns to its pre-PPI baseline.
Based on the research and my own experience, here is what to expect:
- Weeks 1 to 4: This is typically the worst period. Heartburn, regurgitation and increased reflux are common. This is the peak of the rebound effect. Knowing this in advance makes it far more manageable — you’re not panicking that your condition has deteriorated, you’re waiting out a known, temporary pharmacological effect.
- Weeks 4 to 8: Symptoms generally begin to settle. For people who tapered slowly and have the diet and Gaviscon Advance in place, this period is often quite manageable.
- Weeks 8 to 12: For most people symptoms have returned to or below pre-PPI levels by this point. For some, particularly those who were on high doses for a long time, it can extend slightly beyond 12 weeks.
The key variable is whether you taper slowly or stop abruptly. Stopping cold turkey produces a sharper, more severe rebound. A gradual taper smooths out the curve significantly.
Before You Start: Get the Foundation in Place
The single most important thing you can do before starting a PPI taper is to get the low acid diet in place first. I recommend at least 4 to 6 weeks on the diet before you start reducing your dose. Here’s why this matters so much.
When you stop PPIs your stomach is temporarily producing more acid. If you’re also eating acidic foods and drinks during this period, you’re adding dietary acid on top of rebound acid — and it becomes very hard to manage. But if you’ve already significantly reduced dietary acid before starting the taper, the rebound effect hits a system that’s already in a much better baseline state.
Gaviscon Advance (UK version) should also be in place before you start. The sodium alginate in Gaviscon Advance creates a physical raft on top of stomach contents that mechanically prevents acid from reaching the throat — and this barrier protection is particularly valuable during the rebound period when acid production is elevated. More on how to use it in my Gaviscon Advance guide.
In short: sort the diet and Gaviscon first, then start the taper. Don’t try to do everything at once.
How to Taper Off PPIs: A Step-by-Step Approach
The safest way to stop PPIs is to reduce the dose gradually over several weeks, giving the stomach time to readjust at each step before reducing further. The clinical guidelines — including the 2022 AGA expert review and the Canadian deprescribing guidelines — both support a step-down approach, with options including dose reduction, increasing dosing interval, or switching to an H2 blocker as a bridge.
Here’s the approach I recommend based on the research and my own experience:
Step 1: Reduce dose by 50%
If you’re on 40mg, drop to 20mg. If you’re on 20mg, drop to 10mg (or take your 20mg every other day). Stay at this reduced dose for 2 weeks minimum — longer if you feel any significant increase in symptoms. The principle is: only move to the next step when you feel settled at the current one.
Step 2: Every other day dosing
Take your reduced dose every other day rather than daily. Do this for 2 weeks. This step can feel counterintuitive but it gives the stomach periodic days of adjustment without complete withdrawal.
Step 3: Every third day, then stop
Take your dose every third day for 1 to 2 weeks, then stop completely. By this point the stomach has been gradually adjusting for several weeks and the final step is much easier than cold turkey would have been.
The entire process typically takes 6 to 10 weeks depending on your starting dose and how your body responds. The longer you’ve been on PPIs and the higher the dose, the slower and more gradual the taper should be. There’s no prize for rushing it.
If you’re on a capsule PPI like omeprazole: Many omeprazole capsules contain small beads inside that can be separated — you can open the capsule and count out roughly half the beads to approximate a half dose. Ask your pharmacist about lower dose options in your country as some are available over the counter at 10mg or 20mg.
Managing Symptoms During the Taper
Even with a slow taper you’ll likely experience some increase in symptoms, particularly in the first few weeks. Here’s what actually helps:
Gaviscon Advance (UK version) — your main tool. Take it after every meal and before bed throughout the taper. This is doing the job the PPIs were doing — protecting the oesophagus and throat from acid reaching them — but through a physical barrier mechanism rather than acid suppression. It doesn’t cause rebound when you stop it. This is the key medication for managing the transition.
H2 blockers as a bridge. Famotidine (Pepcid) is a weaker acid suppressant than PPIs but can be useful during the taper to take the edge off rebound symptoms. Unlike PPIs, H2 blockers work differently and tolerance tends to develop quickly, so they’re most useful as a short-term bridge rather than a long-term substitute. Note: H2 blockers can also cause a milder rebound so ideally don’t become reliant on them either.
Alkaline water. Drinking alkaline water at pH 8.8 or above throughout the day helps neutralise pepsin in the throat and maintain an alkaline environment. During a PPI taper when acid production is elevated, this is particularly useful as a daily habit.
Meal timing and portion size. Don’t eat within 3 hours of bed. Keep portions moderate — overeating puts pressure on the lower oesophageal sphincter and increases reflux regardless of acid levels. These are basic principles but they matter more during the rebound period than at any other time.
Elevating the head of the bed. If night-time symptoms are a problem during the taper, raising the head of your bed by 15 to 20cm (6 to 8 inches) using bed risers under the legs reduces nocturnal reflux. This is particularly relevant for GERD symptoms during the rebound period.
Common Mistakes to Avoid
Stopping cold turkey. I did this and ended up in A&E twice. The rebound was severe because I went from full suppression to zero overnight. Don’t do it. Always taper.
Starting the taper before the diet is in place. If you’re still eating acidic foods when you stop PPIs, you’re fighting a losing battle. Get the diet right first, then taper.
Mistaking rebound for your condition worsening. This is the most common reason people restart PPIs — they feel worse when they stop and conclude they need the medication. In many cases what they’re feeling is rebound, not underlying disease. If you know this in advance and have a plan for managing symptoms during the taper, you’re far less likely to be derailed by it.
Using H2 blockers long-term as a substitute. H2 blockers are a useful bridge during a taper but they’re not a long-term solution for LPR. The mechanism that causes LPR — pepsin reaching the throat — isn’t addressed by H2 blockers any more than it is by PPIs. Focus on diet and Gaviscon Advance as the sustainable long-term approach.
Frequently Asked Questions
Is acid rebound real or am I just imagining it?
Acid rebound is a well-documented, physiologically established phenomenon. A controlled trial in healthy volunteers with no prior reflux found that 44% developed acid-related symptoms after stopping PPIs — caused by the medication withdrawal, not any underlying disease. A 2024 review in the International Journal of Molecular Sciences confirmed the mechanism is well understood. It is real, it is common, and it is temporary.
How long does PPI rebound last?
Acid rebound typically peaks in the first 2 to 4 weeks after stopping PPIs and resolves within 8 to 12 weeks for most people. How severe and how long it lasts depends on how long you were on PPIs, the dose, and whether you tapered gradually or stopped abruptly. Tapering significantly reduces the severity and duration of rebound symptoms.
Can I stop PPIs if I have LPR?
Yes — and for most people with LPR, coming off PPIs is the right move because PPIs have not been shown to be effective for LPR in clinical trials. The approach is to taper slowly, get the low acid diet and Gaviscon Advance in place before starting, and manage rebound symptoms with the tools covered in this article. If you’re unsure about your specific situation consider a private consultation.
What can I take instead of PPIs for LPR?
The most effective approach for LPR is a combination of the low acid diet, Gaviscon Advance (UK version) after meals and before bed, and alkaline water as your main drink. This combination addresses pepsin directly — which PPIs do not — and has clinical evidence behind it. For the complete picture see my silent reflux treatment guide.
Do I need to tell my doctor before stopping PPIs?
If you’re on PPIs for a documented reason other than LPR — such as a confirmed peptic ulcer, Barrett’s oesophagus, or severe erosive oesophagitis — you should discuss stopping with your doctor first. For people who were prescribed PPIs for LPR or general reflux and are considering stopping, tapering with the approach described here is generally safe, but speaking to your GP about your intention is sensible.
Can rebound make my LPR permanently worse?
No. Rebound acid hypersecretion is temporary. Once it resolves — typically within 8 to 12 weeks — acid production returns to its pre-PPI baseline. The rebound doesn’t cause any permanent change to the stomach or oesophagus. The discomfort during the transition is real but the endpoint is a return to baseline, which for most people with LPR means symptoms that are much better managed with the right diet and medication approach than they ever were on PPIs.
Conclusion
Acid rebound is the main reason people struggle to come off PPIs and the main reason they go back on them unnecessarily. Understanding that it is a temporary, pharmacologically-caused withdrawal effect — not evidence that you need the medication — is the most important mindset shift you can make. Taper slowly, get the diet and Gaviscon Advance in place first, manage symptoms with the right tools during the transition, and give it 8 to 12 weeks. For most people the other side of that is significantly better than where they started.
If you want a complete structured plan for managing LPR without PPIs, check the Wipeout Diet Plan. For personalised guidance on your taper and your specific situation, I offer private consultations.
Related articles:
- The Complete Guide to LPR — Causes, Symptoms and Treatment
- Gaviscon Advance for LPR — Why It Works and How to Use It
- Silent Reflux Treatment — What Actually Works
- LPR Diet — What to Eat, What to Avoid
- Alkaline Water for LPR — Does It Help?
- How I Cured My Silent Reflux
References
- Reimer C, Sondergaard B, Hilsted L, Bytzer P. (2009) “Proton-pump inhibitor therapy induces acid-related symptoms in healthy volunteers after withdrawal of therapy.” Gastroenterology, 137(1):80-87. PubMed PMID 19362552
- Namikawa K, Björnsson ES. (2024) “Rebound Acid Hypersecretion after Withdrawal of Long-Term Proton Pump Inhibitor (PPI) Treatment — Are PPIs Addictive?” International Journal of Molecular Sciences, 25(10):5459. PubMed PMID 38791497
- Targownik LE, Fisher DA, Saini SD. (2022) “AGA Clinical Practice Update on De-Prescribing of Proton Pump Inhibitors: Expert Review.” Gastroenterology, 162(5):1334-1342. PubMed PMID 35183361
- Deprescribing.org / Canadian Deprescribing Network. (2017) “Deprescribing proton pump inhibitors: Evidence-based clinical practice guideline.” Canadian Family Physician, 63(5):354-364. PMC5429051
- Lechien JR et al. (2019) “Efficacy and safety of proton pump inhibitors for chronic laryngitis: A systematic review.” Laryngoscope, 130(5):1173-1189. PubMed PMID 31478201
David Gray
Content Researcher & Author
David Gray founded Wipeout Reflux to address a critical gap in reflux management. His research synthesizes over 100 peer-reviewed studies on laryngopharyngeal reflux (LPR), pepsin biology, and GERD pathophysiology. For LPR specifically—a condition most physicians misdiagnose—his work focuses on pepsin reactivation and why standard PPI therapy fails most patients. He develops evidence-based protocols targeting root causes of both LPR and GERD, integrating emerging research on sphincter dysfunction, dietary interventions, and newer clinical approaches. Wipeout Reflux represents practical application of clinical science for patients seeking real solutions.
Hi David. I took 40 mg. Pantoprazole for 10 weeks and stopped abruptly without tapering off. The doctor said nothing about tapering and I did not know that that was the best way to end the course of PPI’s . Now, a few months later, My reflux is worse than ever and not improving. I won’t be able to see my doc for another month (it takes forever to see a doc around here). Would it be advisable to start taking the PPI’s again for a brief period , say a couple of weeks, then begin the tapering off process for a few weeks with progressively lower doses? Thank you!
Hi Richard, yeah you could go back onto them at a lower dose for example 20mg and then taper it after a couple weeks like you said yes.
Hi David. Thank you so much for your advice on tapering off of PPIs. I’d been on PPIs for well over 10 years. My reflux suddenly worsened at the beginning of 2022 so I was started on a different PPI, pantoprozole and the dose was increased to twice daily which I took for the rest of 2022. Over the years I’d unsuccessfully tried to wean myself off. I found your website in 2023 and decided to try again as I was increasingly concerned about the side effects of PPIs. I did a very slow taper over 3 months, first the morning dose then the evening dose and I’ve been mostly symptom free since then. I cannot thank you enough!! The slow taper plus some of your other suggestions were awesome. Thank you, thank you, thank you!!
Hey Adrienne,
You are most welcome! I love to hear you have been able to stop especially after taking them for quite a long time. Congratulations!
Hello,
Thank you for all this information.
I have been taking ppis for many years( I think more that 15).Despite 20mg a day, I still had daily symptoms – disturbed nights with regurgitation, heartburn etc. I have been following a low acid diet which meant that my symptoms improved dramatically. I decided to wean myself off Esomeprazole. I missed a tablet very 3 days at first, then alternate days. After about 2 successful months, I have started having acid-induced coughing. I have been using Gaviscon Advance but still being woken in the night with reflux.
Is this acid rebound? Can it take 2 months to happen?
I have felt very tempted to go back on daily ppis but desperately want to come off them. I am worried about damage caused by pepsin during this time. How long before it will stop, if it is rebound?
It doesn’t sound like acid rebound because you already had 2 good months. Not to say that’s it’s totally out of the question, there is still a chance for that. But if I was you I would consider what has changed in your life and diet and if they could also be affecting it too.
Thank you for this article. I took over the counter Omperazole for about 4 years. I was taking 2 tablets every morning. Almost 2 months ago it just stopped working out of the blue an I had terrible acid reflux for about a week. Because the two tablets stopped working just all of a sudden I bumped it up to 2 in the morning and 2 at night. After about 2 days I started experiencing very severe side effects. Anxiety, panic attacks, suicidal thoughts, muscle spasms, SEVERE nausea, no appetite. Gastro Dr put me on Nexium and said to stop the omperazole. Side effects continued. I have now tried to take 3 different PPI’s and all have given me horrific side effects out of the blue. I stopped taking all PPI’s almost 3 weeks ago now. My acid reflux if thru the roof. A 10 out of 10 most of the day. I have been taking Cimetidine twice a day and pepto as needed just to get some relief. Does this sound like rebound acidity? I am hoping and praying that it stops. I did have an endoscopy and the Dr said that there were no significant findings on the endoscopy.
Is this rebound acidity and how long should it last with long term use of the PPI’s?
Hi Amy,
Yeah that definitely sounds like acid reflux rebound effect. Do follow my advice here in the article it should make the transititon much easier. Ideally within 1 month things should be back to normal, if not you’ll need to focus on some of these steps I mentioned here.
Hi David,
Thank you for your article! My GI specialist completely disregarded my comment about rebound effect. I’ve never had acid reflux in my entire life and right after stopping omeprazole (40 mg for two weeks) i am experiencing the worse LPR, it’s awful, all day everyday, even with low acidity diet. It’s been 4 weeks and i’m praying for this to pass quickly, this has been hell. Do you think after a 2 weeks i could get a rebound effect? I just stopped it since no one told me to taper them off(((
Hi Karina,
Yes you could still get a rebound after 2 weeks. I think it could last up to 3 months but people usually see an improvement quicker than that.
David
I would like to try this Gaviscon but isn’t there concerns of it containing aluminum?
It is safe to take, especially if only taken in the short term.
Dear David..I often read your site and have done for 3+ years Reason, my son. Emigrated to Canada,sadly for me, was great for 18mths. He started with several problems never having been sick a day in his life! Had throat problems, torso pain and was told initially, stress. Long story short, he was diagnosed LPR having had camera through his nose to upper part of chest. He was also diagnosed,through persistence, all at the same time, kidney stones, and pneumonia eventually,resulting in bi lateral blood clots both lungs. I flew out as a mum would. Thankfully he recovered but is on permanent blood thinners. Riveroxiban as they don’t know why he clotted! EG no DVT. His throat continues, clearing his throat and a feeling of constriction,as if his throat is being squeezed. He was told in Feb this year he has fatty liver disease and was mortified. Doctor said,loose weight, excercise and diet! He’s done that and lost weight and doctor v pleased. However…the LPR…still persists. He,my son,is thinking stress could be major factor. Why wouldn’t he be..he stopped the PPI meds after I talked about what I read on your site. He was recently put on them…Feb…to see if that helped. He is going for an endoscopy…I …am v nervous. Mum thing. I feel the dieting for his liver has helped and wonder if it’s all connected somehow. He can’t pinpoint triggers for his throat which he thought he could with his new diet regime..hence the stress issue. It’s super sad as he is now alone,he and his partner split…so I guess no one to bounce off. I have to say all things considered he does well. Admissions..he started to drink a lot, ate very spicy foods, meat but lots of fish too. All changed. Sorry to have rambled, I thank you for your very interesting and informative site, and if or should you have any comments. A very grateful but anxious mum
Tina……ps he was 37 at the start and is now 41…less worry would be amazing. Let’s hope.
Yeah I’d definitely suggest to look into my wipeout diet plan if that’s something he could commit too. It’s something that will most likely give him an improvement if he follows through with it. Try not to worry about the endoscope, I have had it done and its quite simple and straightforward. And yes stress definitely plays an important rule, lowering it should help.
Hi:
Is there anything you can do to help if you did stop cold turkey and are suffering from rebound?
Thanks
Sheila
Take something like Gaviscon to aid you from coming off the meds if you can and avoid trigger foods too which is very important.
I am just trying to come off omeperazole which was prescribed for gastritis. I have been taking it for 6 weeks now ( 20mg once a day). I have cut down to 10mg every other day. I seem to get dreadful hunger pains and a very gurgly tummy just before meal times. Could this be rebound? Also, can acid rebound CAUSE gastritis or a stomach ulcer? Thank you.
Yes it could be related to rebound. I’m not sure rebound can cause them things but it’s always plausible, but if you taper off it I imagine it almost definitely will not.
Hi David,
I went on PPIs for a feeling like something was stuck in my throat. Well, let me just tell you, after going on and off the medicine for a few weeks at a time and stopping, I have more acid reflux symptoms now than ever. I have a sour taste in my mouth, chronic burning and the lump sensation has not gone away. I’ve been off all medicine for 5 weeks. Does this sound like rebound? I read it can take 8-24 weeks for levels to go back to normal.
Hi Shana,
Yes it does sound like rebound, as I mentioned in this article try to keep other acidity lower with diet and other aids like gaviscon until it settles down more. I haven’t heard that timeframe before but I could imagine it to be true.